
Laser Treatment Center for Anal Conditions
Colorectal Cancer Treatment Center
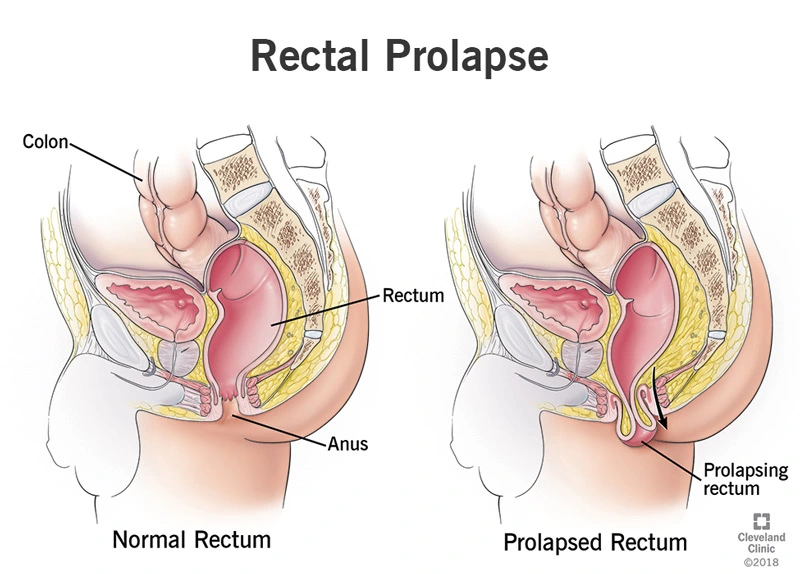
Rectal prolapse refers to the abnormal protrusion of part of the rectum through the anal canal.
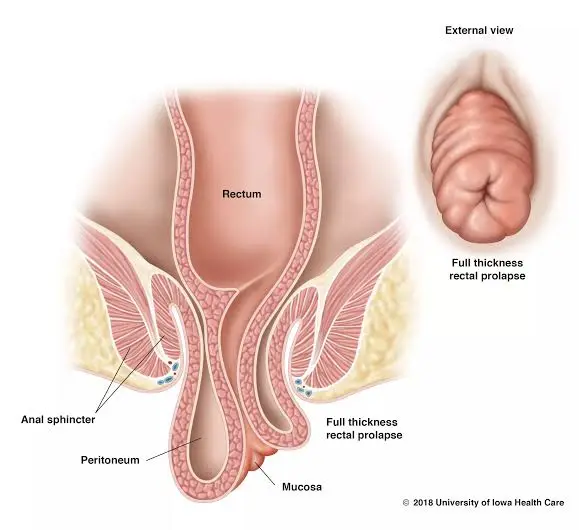
This protrusion may involve only the superficial mucosal layer or the full thickness of the rectal wall.
In some cases, internal intussusception occurs—where the rectum folds inward on itself without protruding externally. Rectal prolapse may be temporary at first but can become persistent over time, significantly affecting quality of life.
The rectum is the final segment of the large intestine, measuring about 12–15 centimeters in length, located just before the anal canal.
Its primary function is to temporarily store stool and provide the conditions necessary for controlled defecation.
Important note: Having one or more risk factors does not necessarily mean prolapse will occur; these factors only increase the likelihood.
Diseases that weaken the nerves controlling the pelvic floor—such as spinal cord injuries or peripheral neuropathies—can impair the supportive tissues and disrupt the mechanisms that keep the rectum in place.
Prior pelvic surgeries, adhesions, or chronic inflammatory conditions can alter the architecture of the supporting structures.
Some individuals, due to connective tissue disorders or age-related decline, experience reduced collagen quality and weakening of connective tissues. This leads to decreased ligament strength and a significantly increased risk of prolapse.
Summary of the Mechanism
A combination of repeated straining, direct injury (such as childbirth trauma), and deterioration of supportive tissue quality gradually displaces the rectum from its normal position, eventually allowing it to protrude.
Patients typically report one or more of the following:
When these symptoms become recurrent or progressive and begin to affect quality of life, prompt evaluation is important.
Examination is performed both at rest and during straining to visualize any prolapse.
A digital rectal examination assesses sphincter tone and checks for ulceration or inflammation.
This is the first and most important step in evaluation.
A paste with stool-like consistency is inserted into the rectum by the physician or radiologist. The patient then sits on a special commode-like chair while the fluoroscopy machine records real-time imaging. The patient is asked to take several deep breaths and then strain so that the actual process of filling and emptying can be captured. This study shows when the prolapse occurs, whether internal intussusception is present, the depth of any rectocele, and the degree of perineal descent.
Preparation usually involves simple instructions from the radiology center or a light enema.
Dynamic MRI evaluates the same process without radiation and with greater soft-tissue detail. MRI provides better visualization of the mesorectum, fascia, the relationship with the bladder and vagina, and internal intussusception.
For patients with multicompartment involvement, a history of prior surgery, or incontinence, MRI supplies essential information for surgical planning.
Endoanal ultrasound provides a direct image of the internal and external sphincters and can reveal childbirth-related tears or scarring. Manometry measures resting and squeeze pressures of the sphincters and shows how well the muscles are functioning.
Together, these findings determine whether the patient also requires sphincter repair.
Before surgery, colonoscopy is essential to rule out synchronous polyps or tumors. If the patient has not previously undergone colonoscopy, it is typically scheduled.
Decision-making is based on the severity of symptoms, the type of prolapse (mucosal or full-thickness), sphincter function, and the patient’s overall condition. If the prolapse is mild and does not impair function, non-surgical management is attempted first. If the prolapse is full-thickness, symptomatic, or causing ulceration or incontinence, surgery is usually the best option.
Non-Surgical Treatments and Home Care (Low-Cost and Effective Measures)
These measures are especially effective in early stages and for preventing progression.
These procedures are generally chosen for older patients or those who cannot tolerate abdominal anesthesia. The two main techniques are:
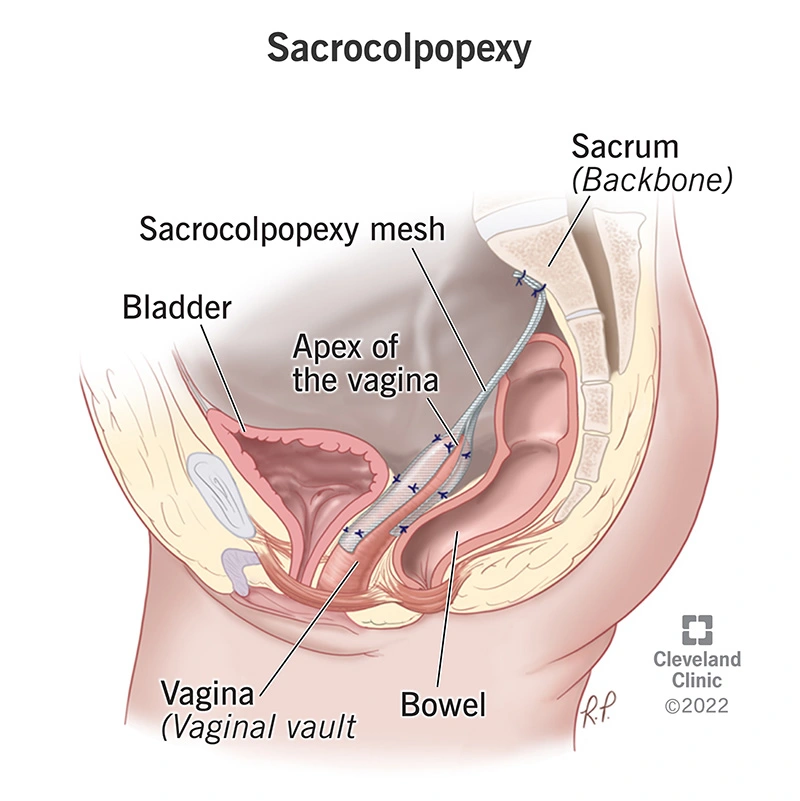
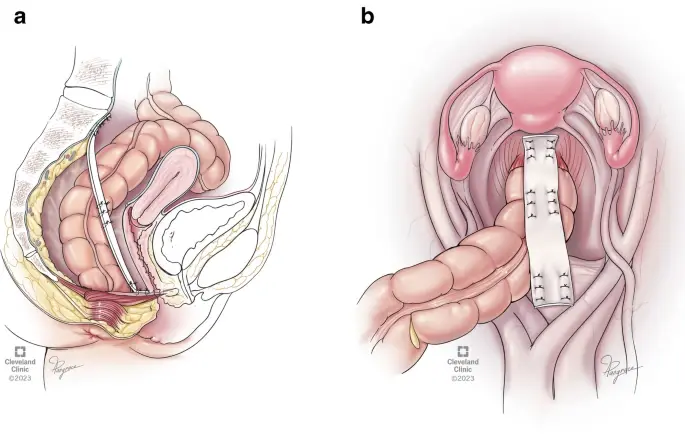
Abdominal procedures generally provide more durable results and lower recurrence rates in younger patients and those who are good candidates for anesthesia. The two major techniques are:
Resection Rectopexy In this technique, in addition to rectopexy, a portion of redundant sigmoid colon is removed.
It is suitable for patients with a long sigmoid colon and refractory constipation but carries risks related to the anastomosis (bowel connection), making surgeon experience essential.
Summary Comparison : Abdominal methods generally offer more stable functional outcomes, and laparoscopic/robotic techniques can reduce complications and length of stay.
However, final selection must be made by a multidisciplinary team after reviewing dynamic imaging and the patient’s overall condition.
In selected cases of mucosal prolapse or internal intussusception associated with obstructed defecation, techniques such as STARR or stapled mucosectomy may be helpful.
However, they are usually insufficient for full-thickness prolapse, and patients must be chosen very carefully.
No—if the prolapse is very mild and asymptomatic, surgery is not necessary. However, full-thickness and symptomatic prolapse usually requires surgical treatment.
For appropriate patients, yes.
Laparoscopic or robotic techniques provide enhanced visualization and magnification, along with finer instruments that facilitate preservation of pelvic nerves.
Postoperative pain is typically less, and return to daily activities is faster.
The final decision depends on the patient’s condition and the experience of the surgical center.
If you experienced a third- or fourth-degree tear, or if you have had symptoms of leakage or a sensation of prolapse since childbirth, you should definitely consult a colorectal surgeon.
Timely primary repair and proper follow-up significantly improve outcomes.
A high-fiber diet with adequate fluids, stool softeners when needed, avoiding prolonged straining, and treating chronic cough are important steps.
Performing pelvic floor exercises at home is also helpful.
Many patients experience significant improvement, although in some cases minor changes in bowel habits may persist.
The care team will discuss realistic expectations with you before surgery.
An anal fissure is a painful tear in the skin of the anus, usually accompanied by pain and bleeding.
Most cases improve with dietary changes, stool softeners, and warm baths.
If it does not heal within 6–8 weeks, treatments such as medicated ointments, Botox injection, or a minor procedure called lateral internal sphincterotomy may be recommended.
Most patients recover with appropriate therapy; choosing the right treatment depends on a thorough examination and consultation with a colorectal surgeon.