
Laser Treatment Center for Anal Conditions
Colorectal Cancer Treatment Center
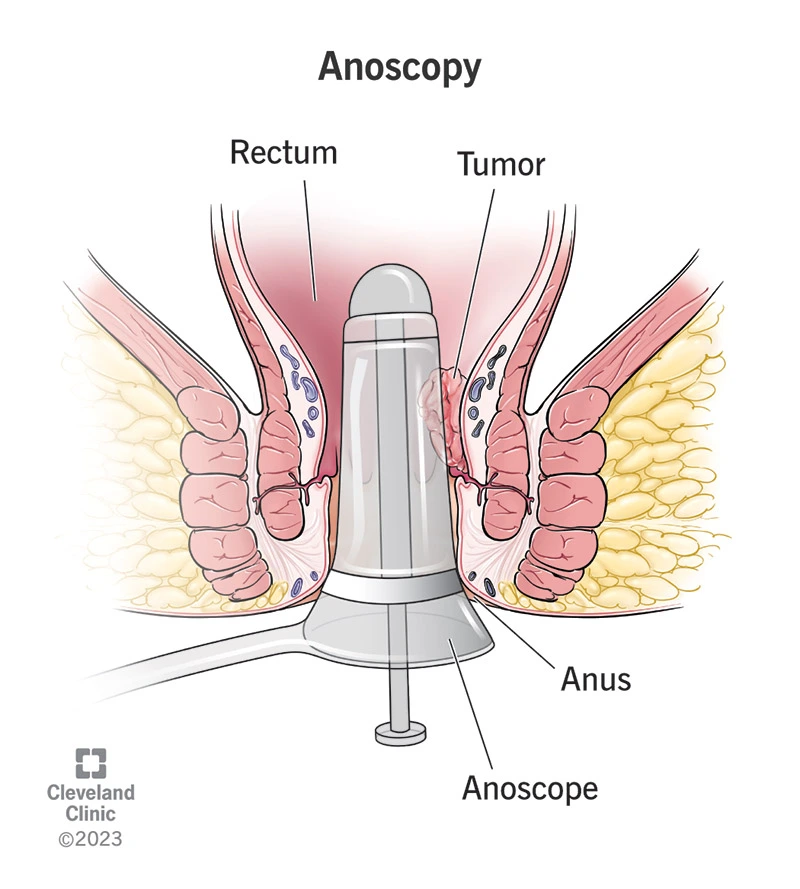
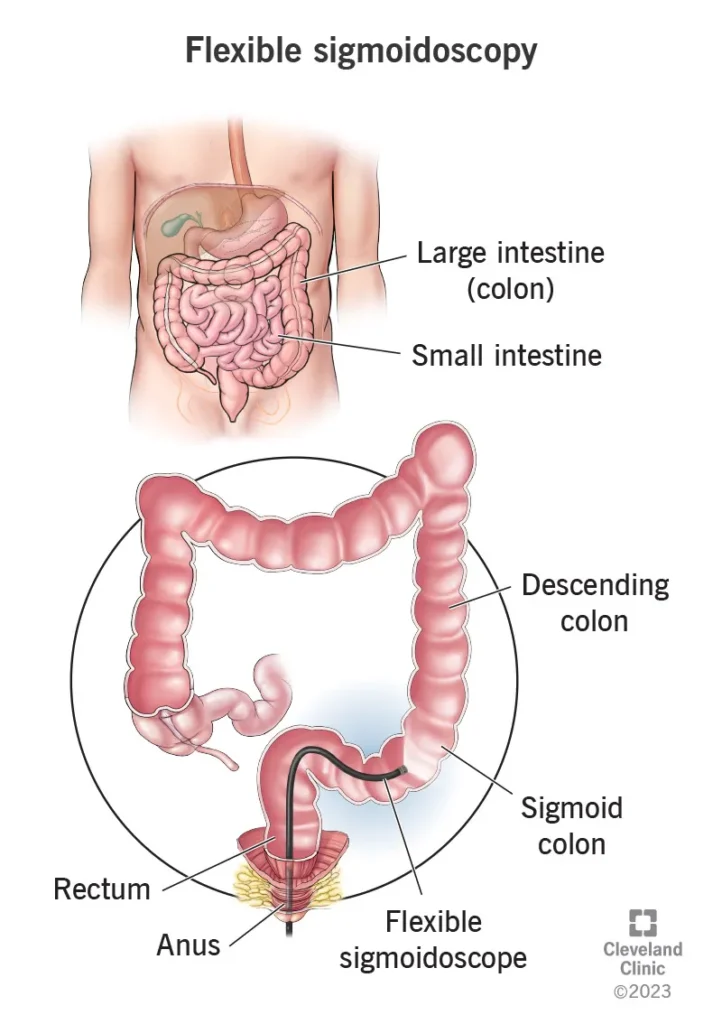
The rectum is the final part of the large intestine, located about 10 to 15 centimeters above the anus. Rectal cancer refers to the uncontrolled growth of malignant cells in this area. Because the rectum is situated within the confined space of the pelvis and lies close to the nerves, bladder, vagina, and reproductive structures, its treatment is technically more complex. Management often requires a combination of radiation therapy, chemotherapy, and surgery, all coordinated by a multidisciplinary medical team.
Rectal cancer accounts for about 30–35% of all colorectal cancers worldwide and is considered one of the major challenges in colorectal surgery. In Western countries, its incidence has been declining due to widespread colonoscopy screening programs. However, in developing countries—including Iran—the incidence continues to rise.
In Iran, the proportion of rectal cancer relative to all colorectal cancers is similar to global statistics, but a notable characteristic is the younger age of onset. A significant number of Iranian patients are under 50 years old at the time of diagnosis.
Several factors increase the risk of developing rectal cancer. The most important include:
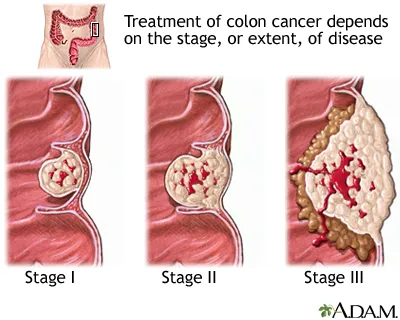
Most colorectal cancers follow the adenoma–carcinoma sequence:
A benign polyp forms first; over time, genetic mutations accumulate within it, and some polyps gradually become malignant. This process typically takes several years, which is why removing polyps during colonoscopy is both preventive and essential.
Warning signs that should not be ignored include:
Any persistent symptom warrants medical evaluation — even in younger individuals.
Why it matters: Pelvic MRI provides crucial information about: Depth of tumor invasion into the rectal wall (T stage) Tumor proximity to or involvement of the circumferential resection margin (CRM) Presence of extramural vascular invasion (EMVI) Suspicious regional lymph nodes
These findings determine whether preoperative chemoradiotherapy is needed and guide surgical planning. The MRI report should clearly specify: Distance to CRM EMVI status Tumor distance from the anal verge
PET-CT:
Used in selected cases, such as when findings are unclear or to assess treatment response. Molecular analysis: Pathology samples are typically tested for: MSI/MMR statusKRAS/BRAF mutationsOther relevant markersThese results influence the selection of targeted therapies and immunotherapy.
Treatment decisions in rectal cancer are complex and must be individualized. Each patient receives a coordinated plan developed by a multidisciplinary team, typically including a colorectal surgeon, a radiation oncologist, and a medical oncologist.
There are two commonly used approaches:
The purpose of neoadjuvant therapy is to reduce tumor size, lower the risk of local recurrence, and enable surgery with clear margins.In some cases, newer protocols known as Total Neoadjuvant Therapy (TNT) incorporate systemic chemotherapy before surgery to enhance rates of complete response. These approaches are used in specialized centers with careful patient selection.
For individuals at average risk, screening should begin at age 45.
If you have a family history of colorectal cancer or a genetic syndrome, screening typically starts 10 years before the youngest affected family member’s age at diagnosis, or at age 40—whichever comes first.
Consult a gastroenterologist or a genetic counseling center for personalized guidance.
The report should specify the distance from the tumor to the circumferential resection margin (CRM), the presence or absence of EMVI, the T stage, the tumor’s distance from the anal verge, and any suspicious lymph nodes. These findings are essential for determining the appropriate treatment plan.
It refers to chemoradiation given before surgery to shrink the tumor and increase the likelihood of sphincter preservation or achieving clear surgical margins.
Neoadjuvant therapy is typically used for locally advanced tumors or those that threaten the circumferential resection margin (CRM).
No. If all liver lesions can be surgically removed or locally controlled, and the patient’s overall condition is suitable, metastasectomy can be performed with curative intent. This decision is made by a multidisciplinary team.
Both techniques provide excellent oncologic outcomes in well-equipped centers. Robotic and laparoscopic approaches offer advantages in the narrow pelvic space, allowing for more precise dissection and better nerve preservation.
The choice depends on the surgical team’s experience and the patient’s specific circumstances.
Rectal cancer is a condition that, in many cases, is treatable or manageable when detected early. Diagnosis is based on colonoscopy and pelvic MRI, and treatment decisions typically involve a combination of chemoradiation and surgery using the TME technique.
In modern centers, laparoscopic or robotic approaches—and, in selected cases, local excision techniques such as TEM, TAMIS, or TEO—can offer effective treatment with better functional outcomes and fewer complications. However, all of these options require an experienced team and careful patient selection.
Any major intervention—especially complex surgery—should be guided by a specialized colorectal surgeon and managed within a multidisciplinary team.