
Laser Treatment Center for Anal Conditions
Colorectal Cancer Treatment Center
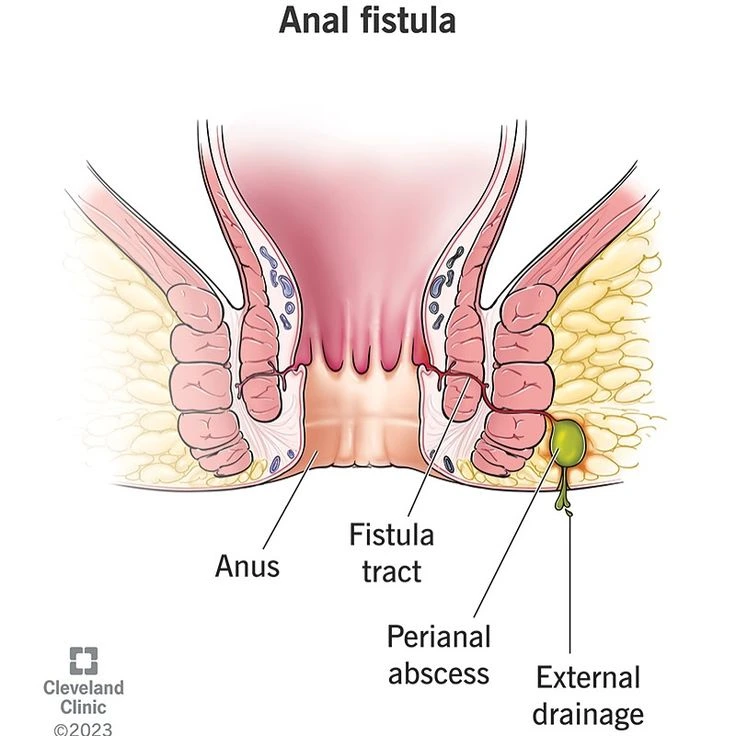
An anal fistula is an abnormal tract or tunnel that forms between the internal space of the anal canal—typically originating from a cryptoglandular site or following an anorectal abscess—and the perianal skin. In simple terms, it is a “purulent pathway” that opens from inside the rectum to the outside, and is usually associated with recurrent discharge, pain, or perianal irritation. The goal of treatment is to close this tract while preserving sphincter function.
Proper sphincter function determines the risk of postoperative incontinence; the less muscle divided, the lower the likelihood of dysfunction.
An anal fistula is a pathological tract or tunnel between the internal space of the anal canal and the perianal skin, typically developing after an anorectal abscess.
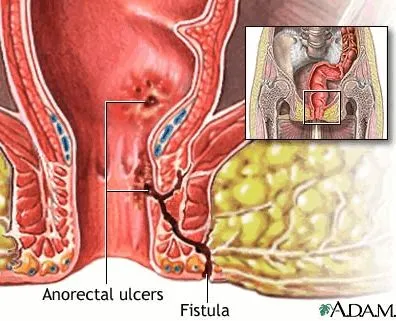
The typical sequence begins with obstruction or infection of a crypt gland, leading to the formation of a localized abscess. If the abscess is not adequately drained, or if purulent material extends along areas of tissue weakness, a tunnel-like tract may persist after drainage, maintaining communication between the internal mucosa and the external skin—this persistent tract is the fistula.
In Crohn’s disease, the inflammatory process within the bowel wall can directly generate fistulas without a clearly defined preceding superficial abscess.
c) Additional Laboratory Tests
A key principle is that treatment aims to close the fistula tract while minimizing sphincter injury and preserving continence. The choice of technique depends on the type of fistula (simple or complex), the location of the internal opening, the condition of the sphincter complex, and the presence of underlying diseases such as Crohn’s disease.
(Approximate ranges based on pooled data from review studies; presented as general estimates.)
Factors associated with treatment failure or recurrence include complex or branching fistulas, a history of Crohn’s disease, active infection, incomplete identification of the internal opening, and inadequate management of the sphincteric component.
In most cases, yes. Persistent discharge and ongoing infection increase the risk of complications, including incontinence. In patients with Crohn’s disease or certain special conditions, initial medical therapy or placement of a seton for drainage may be sufficient before considering definitive surgery.
Incontinence may occur if an inappropriate technique is chosen or if an excessive portion of the sphincter complex is divided. For this reason, sphincter-preserving procedures and management by a colorectal surgeon are essential in complex fistulas.
Depending on the degree of inflammation and the presence of a seton, a waiting period of several weeks to a few months is typically required to allow inflammation to subside and to optimize conditions for definitive repair.
They can be managed, but treatment often requires a combination of medical therapy (such as anti-TNF agents) and staged surgical procedures, and recurrence is more common than in non-Crohn’s fistulas.
Fistula-mapping MRI is the most accurate method for delineating fistula tracts and planning surgical management.
An anal fistula is an abnormal tunnel connecting the inside of the anal canal to the surrounding skin, typically developing after an anorectal abscess. Its main symptom is recurrent drainage of pus or bloody fluid. Diagnosis relies on clinical examination and detailed imaging, particularly MRI.
The goal of treatment is to close the tract while preserving continence. Fistulotomy is effective for simple fistulas, whereas sphincter-preserving techniques (such as LIFT, advancement flap, seton placement, or endoscopic approaches) are preferred for complex cases.
Patients with Crohn’s disease or other underlying conditions also require concurrent medical therapy. Collaboration with a colorectal surgeon and a multidisciplinary team improves outcomes and enhances the likelihood of successful treatment.