
Laser Treatment Center for Anal Conditions
Colorectal Cancer Treatment Center
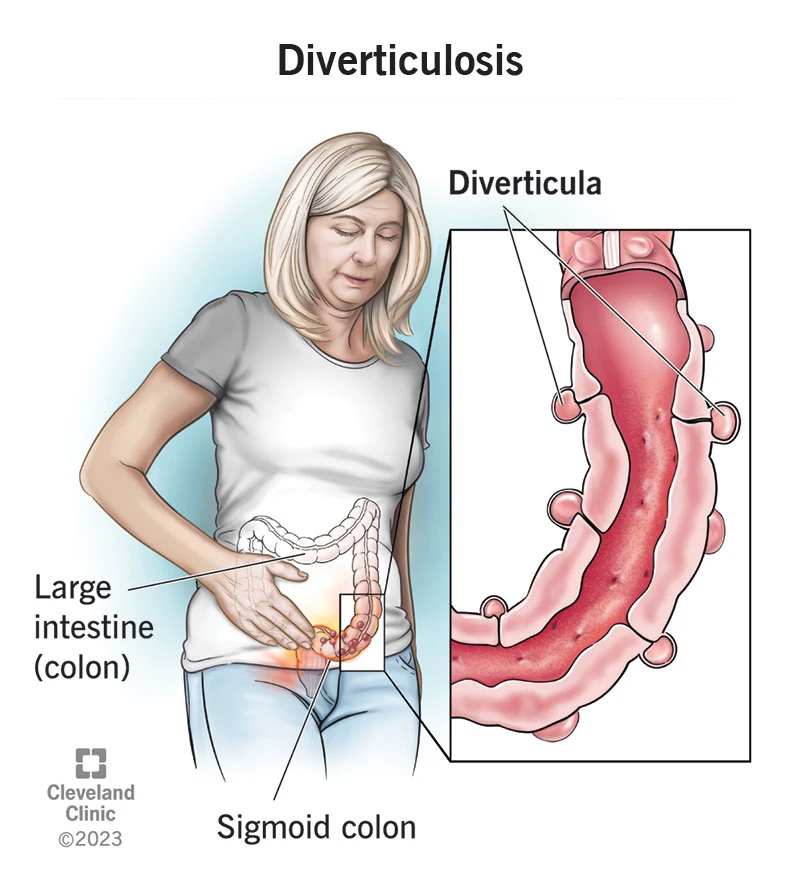
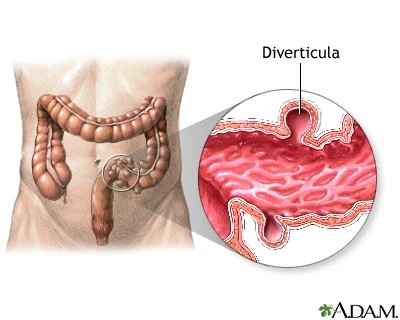
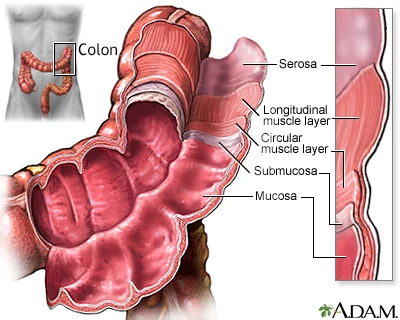
Diverticulosis refers to the presence of multiple small pouches (diverticula) in the large intestine or colon, which protrude outward from the inner layers of the large intestinal wall. When these pouches become inflamed or infected, it is called diverticulitis.
Social and lifestyle factors (diet, activity, obesity) play a significant role in its prevalence.
Chronic use of certain medications such as NSAIDs (non-steroidal anti-inflammatory drugs like ibuprofen, naproxen, aspirin) which can make the mucosa more vulnerable.
In some cases, genetic predisposition or connective tissue disorders play a role.
Mild symptoms: vague or mild discomfort in the lower left abdomen, bloating, or changes in bowel habits.
Complicated symptoms: If an abscess, fistula (an abnormal tunnel between the intestine and bladder or skin), or perforation occurs, severe pain, high fever, generalized abdominal tenderness, or signs of shock may be present.
Surgery is indicated for the management of the following complications:
Not necessarily. There is no strong evidence that eating seeds or nuts triggers diverticulitis. It is generally recommended to follow a high-fiber, well-balanced diet, and to limit any specific foods that cause individual discomfort.
No. In uncomplicated cases without systemic symptoms, supportive care and close follow-up are usually sufficient. Antibiotics are required when there is fever, immunosuppression, or signs of complicated infection. The decision is based on clinical evaluation and imaging findings.
Diverticulosis itself is not considered a cause of cancer; however, after an episode of diverticulitis, it is recommended to undergo colonoscopy once recovery is complete (usually after 6–8 weeks) to rule out other underlying lesions.
Surgery is indicated in cases of perforation, peritonitis, abscesses that cannot be controlled with drainage, symptomatic fistulas or obstruction, and in patients with recurrent, severe episodes that significantly impair quality of life.
A high-fiber diet, adequate hydration, regular physical activity, weight control, and avoiding long-term use of NSAIDs are effective measures to reduce the risk.
Diverticulosis refers to the presence of small pouches in the colonic wall, which are often asymptomatic. Adequate fiber intake, regular physical activity, and prevention of constipation can help reduce the risk of complications. If one of these pouches becomes inflamed or infected, abdominal pain and fever may occur, and treatment—depending on severity—can range from supportive care to antibiotics, drainage, or surgery.