
Laser Treatment Center for Anal Conditions
Colorectal Cancer Treatment Center
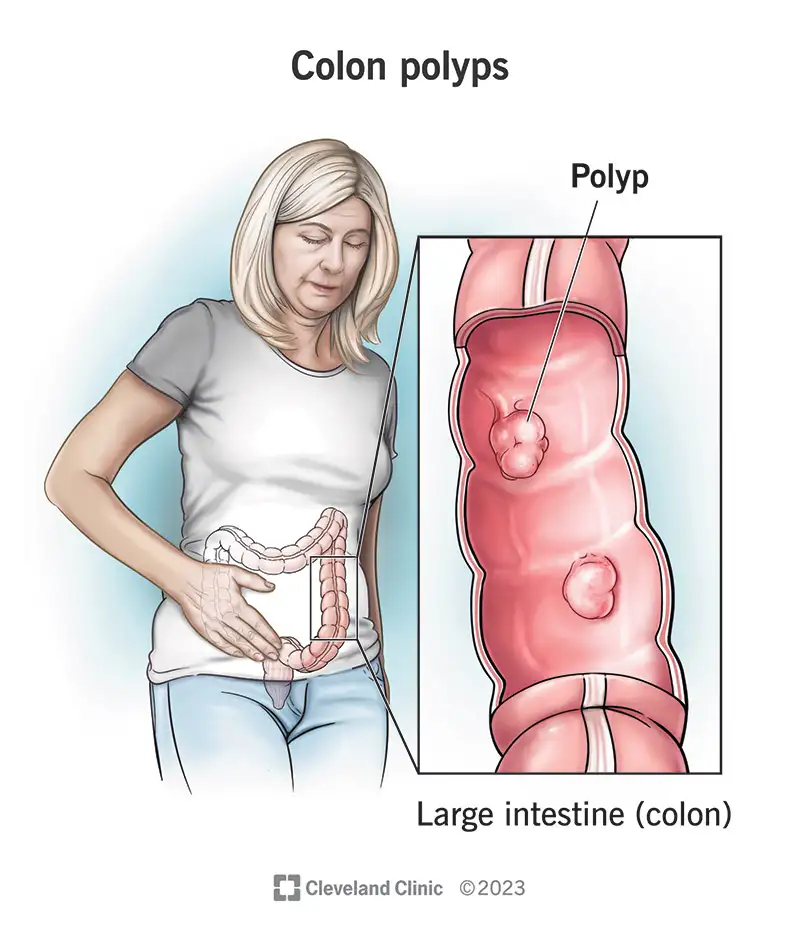
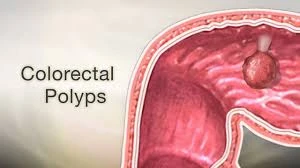
A colon polyp is a growth or “polyp” on the inner lining of the large intestine (mucosa). Many polyps are asymptomatic and are only discovered during a colonoscopy, but some types can develop into cancer over years. Detection and removal of polyps is the most important way to prevent colorectal cancer. The colon is lined internally with a layer called the mucosa. Polyps grow out of this mucosa. When we talk about “seeing a polyp,” we mean seeing this mucosa and any abnormal growth on it.
Sessile: A polyp that is flat and attached directly to the mucosal surface; more experience is needed for its removal.
Serrated lesions: The word “serrated” means “saw-toothed”; under the microscope, the edges of these polyps resemble the edge of a saw. This characteristic causes their molecular growth pathway to be different from classic adenomas, and some of them, especially when large or in the right colon, have a higher chance of progressing to cancer. Therefore, when pathology says “serrated,” we must be more vigilant.
Since most polyps are asymptomatic, adherence to screening programs (colonoscopy or stool tests) is vital.
Most small polyps are asymptomatic. Larger polyps may cause blood on the toilet paper or hidden blood in the stool, which can be detected by a FIT test or fecal occult blood test, or lead to iron deficiency anemia. Chronic changes in bowel habits or obstructive problems are very rare and occur mostly in very large polyps.
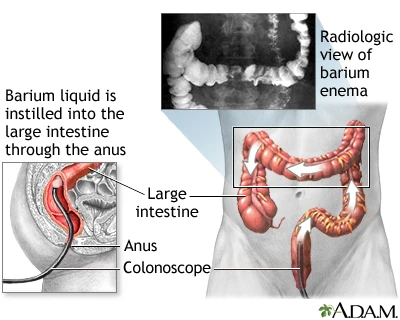
A type of CT scan that creates a three-dimensional view of the inside of the colon through computer reconstruction. Before the scan, air or gas is introduced into the colon to distend the wall, and then images are taken and reconstructed in three dimensions.
Advantage/limitation: It is less invasive and is a reasonable alternative for people who do not want or cannot undergo colonoscopy. If CT colonography shows a significant polyp, a subsequent colonoscopy is usually required to remove the polyp. This means CT is a good diagnostic tool but is often not a simultaneous therapeutic one.
These tests detect hidden blood in the stool and are useful for population screening; if the test is positive, the next step is colonoscopy.
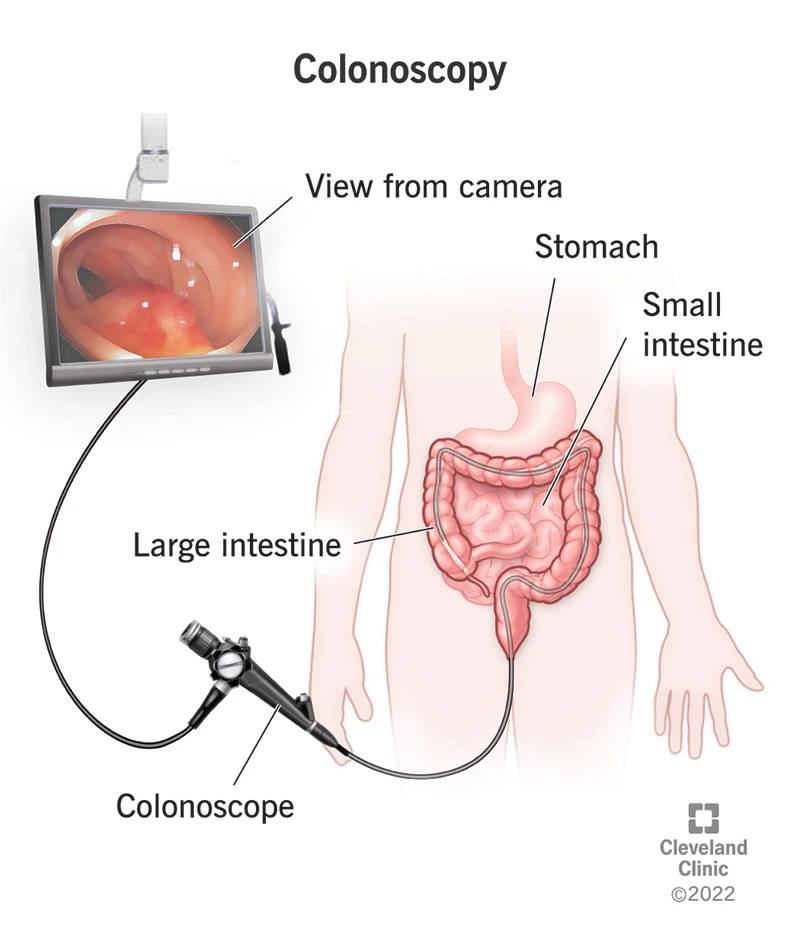
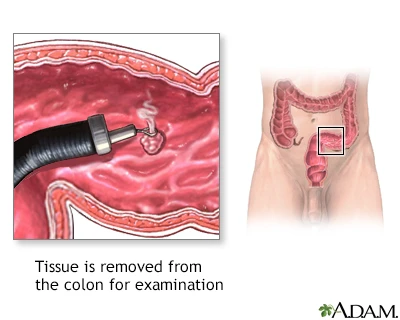
A snare is a thin wire loop that passes through the colonoscope channel. The physician places the loop around the base of the polyp and tightens it. Then, the loop is pulled to separate the polyp; if necessary, a controlled electrical current is used to both cut and simultaneously control bleeding.
Hot snare: With electrical current; used for larger polyps or those with thick stalks and simultaneously helps with hemostasis.
For large sessile or flat polyps, fluid is first injected under the polyp (a fluid similar to saline + a small amount of dye) to lift and separate the polyp from the underlying layer, making it easier for the snare to grasp the base. Then, the polyp is removed with the snare either as a single piece or piecemeal.
Practical note: If the polyp is very extensive, piecemeal removal may be performed, which requires careful pathology follow-up and repeat endoscopy.
Logic: Botox causes temporary and relative paralysis of the internal sphincter muscle, reduces tone, and allows for healing.
How it’s performed: In the office or operating room, it is performed with injections in 2-3 points into or beside the internal sphincter; usually requires local anesthesia and is done as an outpatient procedure.
Success rate: Reviews have reported healing rates of approximately 60-77% (depending on series and studies); however, a significant percentage of patients experience recurrence in the long term and sometimes require repeat injections or surgical intervention. Major complications are rare, and temporary gas/leakage may occur.
Every removed sample is sent to pathology to be examined for the exact type, presence of dysplasia (low or high grade), structural components (such as the presence of a “villous” component), and the resection margins. This report determines the follow-up plan (intervals for repeat colonoscopy).
Hyperplastic polyps are usually benign, but adenomatous polyps (adenomas) are clinically significant.
Adenomas are considered precancerous lesions and increase the risk of developing colon cancer.
A detailed assessment of size, degree of dysplasia (benign or malignant), and completeness of removal is essential for determining the follow-up and subsequent screening schedule.
Proper bowel preparation is the key to a complete view; here is a practical and understandable plan for the patient:
A few days before (2-3 days): Start with a light diet; limit high-fiber or grainy foods as much as possible (such as whole grains, raw vegetables, nuts). If you are taking any specific medications (anticoagulants, antiplatelets), be sure to coordinate with your doctor beforehand; some medications may need to be temporarily stopped or replaced.
The day before the test (morning to evening): Drink only clear liquids (water, clear broth, tea without milk, strained fruit juice without pulp, clear-colored gelatin). Avoid dark-colored beverages (such as red juice).
The night before and split-dose cleansing solution instructions: The best method is usually split-dose; this means consuming half of the cleansing solution the night before and the other half a few hours before your appointment (usually 4-6 hours before). This schedule results in better cleansing and more comfort.
Common solutions: Polyethylene glycol (PEG) (non-absorbable solution); or smaller combination solutions containing sodium picosulfate and electrolytes. The choice of solution varies depending on your medical history (e.g., kidney failure, heart problems) and the center’s recommendation.
Important note for diabetics: Insulin and oral medications may need adjustment; coordinate the exact plan with your doctor and the anesthesia team beforehand.
On the day of the test: Fasting is usually required for several hours beforehand; take your essential medications as directed by your doctor. Be sure to have a driver with you, as sedation is often administered.
If the bowel is not properly cleansed, the colonoscopy may be incomplete and may require repeating the procedure. Therefore, the importance of strict adherence to the prep cannot be overstated.
Large serrated polyp (≥10 mm) or multiple serrated polyps → Closer surveillance (e.g., 3 years).
Generally, yes; because determining the type and risk is only possible with microscopic examination, and removing the polyp prevents it from turning into cancer.
No; having a polyp does not mean you will get cancer. Many polyps are benign. Our goal is to identify and remove polyps that are at risk of transformation to prevent cancer.
If you experience significant bleeding, fever, severe abdominal pain, or sudden discharge of fluid or blood after the procedure, contact us immediately. Also, if the pathology report indicates tumor invasion or significant dysplasia, further action is needed.
Most patients tolerate the procedure well with sedation or light anesthesia and do not experience significant discomfort. After the procedure, you may feel some bloating or mild pain, which is usually temporary.
If you have received sedation, do not drive for 24 hours and have a companion.
A polyp is a small growth on the inner wall of the large intestine. Most polyps do not pose an immediate risk, but some can turn into cancer over time. Colonoscopy is the best method for finding and removing them. Proper preparation before colonoscopy and follow-up according to the pathology report are two key points.