
Laser Treatment Center for Anal Conditions
Colorectal Cancer Treatment Center
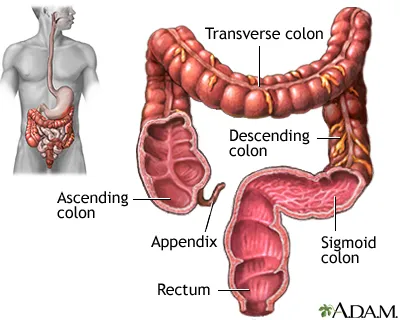
Transverse colon cancer refers to the abnormal growth of cells in the middle portion of the large intestine, which runs horizontally across the upper abdomen from right to left. This growth typically begins in the inner lining of the bowel (the mucosa) and may extend into deeper layers, spread to lymph nodes, or reach other organs.
Transverse colon cancer accounts for about 10% of all colorectal cancers. Epidemiologically, it is less common than right-sided or sigmoid colon cancers, but due to its anatomical location, it may present with vague symptoms such as diffuse abdominal pain or mild changes in bowel habits, making early diagnosis more challenging. Globally, its proportion has remained relatively stable; in Iran, reports indicate a relative increase over the past decade, although it remains less frequent than cancers in other colonic segments.
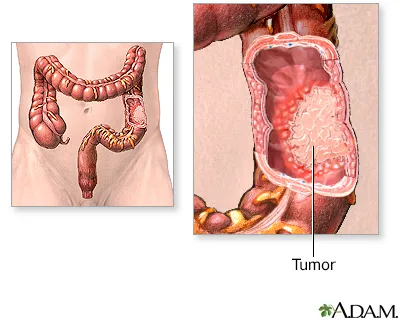
The process begins when cells in a localized area acquire genetic alterations; these cells gradually develop abnormal growth and form a polyp. Over time, with additional mutations, the polyp may transform into a tumor. The tumor can then invade the bowel wall and spread through lymphatic or blood vessels to lymph nodes (small filtering structures in the body that are often the first sites of cancer spread) or to other organs.
Transverse colon cancer often produces no symptoms in its early stages, or its symptoms may be vague. Common manifestations include:
In more advanced stages: marked abdominal bloating, nausea, or bowel obstruction (if the tumor blocks the passage of stool).
Key point for patients: New-onset iron-deficiency anemia in adults must be taken seriously, and its source — which may be gastrointestinal — should be thoroughly investigated.
Questions the physician may ask include: duration and severity of pain, bowel movement pattern, constipation or diarrhea, pregnancy/childbirth history, use of anticoagulant medications, and warning signs (weight loss, fever, significant bleeding, systemic symptoms). This information is essential for determining the need for further evaluation.
A careful inspection of the perianal skin usually reveals the diagnosis; fissures are most commonly seen in the posterior midline. A digital rectal examination (DRE) is performed only if the patient can tolerate it or under local anesthesia.
After initial pain control, simple anoscopy helps visualize the fissure location and any associated papilla or hemorrhoids. Proctoscopy is used to assess higher regions of the anal canal or rectum.
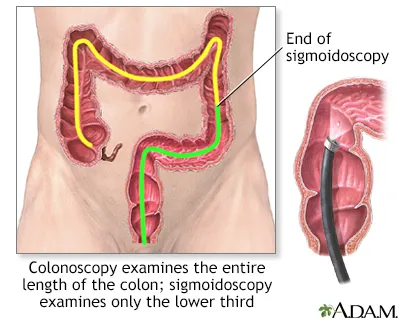
If the fissure is atypical—non-midline, multiple, resistant to treatment, or accompanied by warning signs (such as weight loss or long-standing changes in bowel habits)—a colonoscopy is required to rule out inflammatory bowel disease or more proximal lesions.
This is important because not all fissures require colonoscopy, but in unusual cases or in patients over 40, a full evaluation of the colon is recommended.
In patients who are candidates for procedures that affect sphincter tone (such as botulinum toxin injection) or when evaluating the cause of incontinence before surgery, anorectal manometry measures resting and squeeze pressures of the sphincter and assists in treatment planning.
The tumor’s location creates some practical differences (such as the type of surgery or early symptoms), but the general principles of diagnosis and treatment are similar.
Screening and follow-up depend on your age and family risk. If you are over 50 or have a family history of colorectal disease, you should discuss an appropriate screening plan with your physician.
Many patients return to normal life, but in the first days or weeks there may be temporary changes in bowel frequency or energy levels.
High fever, sudden and severe abdominal pain, heavy bleeding, or pus/discharge from the wound are danger signs and require immediate medical attention.
A high-fiber diet, regular physical activity, maintaining a healthy weight, quitting smoking, and participating in screening programs as recommended by your physician all help reduce the risk.
Transverse colon cancer is a mass that develops in the middle portion of the large intestine. It may begin gradually and without symptoms; fatigue, weight loss, or changes in bowel habits can be early signs. Diagnosis is confirmed through colonoscopy and biopsy, and surgery is usually the first step in treatment. Depending on pathology findings, chemotherapy or targeted therapies may also be added. Regular follow-up and coordinated team-based care provide the best chance for controlling the disease.