
Laser Treatment Center for Anal Conditions
Colorectal Cancer Treatment Center
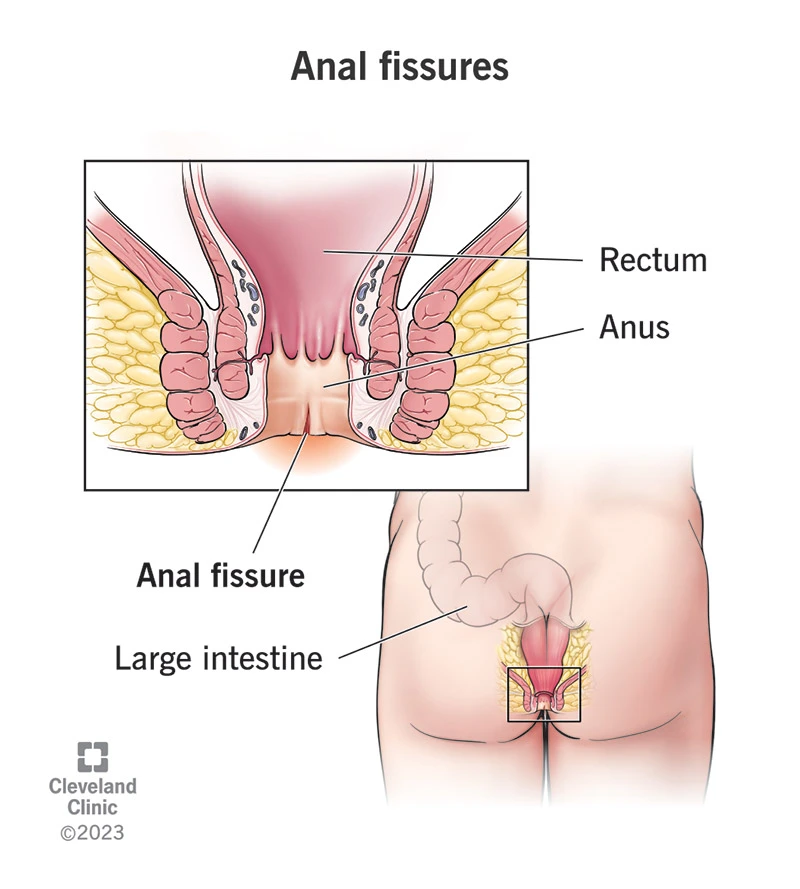
An anal fissure is a longitudinal tear in the delicate skin lining the anal canal (the anoderm).
This tear causes sharp pain during bowel movements and bright red bleeding.
A fissure may be acute (recent and short-term) or chronic (lasting more than 6–8 weeks, often with fibrotic edges or a sentinel skin tag).
Several factors work together to create a cycle that prevents proper healing:
The result of this cycle is: pain → sphincter spasm → reduced blood flow → impaired healing → worsening pain.
If the pain is too severe and the patient is fearful of examination, the evaluation can be performed under local anesthesia.
Key questions include: the duration and severity of pain, bowel movement patterns, presence of constipation or diarrhea, pregnancy or childbirth history, use of anticoagulant medications, and any warning signs such as weight loss, fever, significant bleeding, or systemic symptoms. This information is essential for determining whether further evaluation is required.
A careful inspection of the perianal skin usually confirms the diagnosis; fissures are most commonly found in the posterior midline. Digital rectal examination (DRE) is performed only if the patient can tolerate it or if it is done under local anesthesia.
After initial pain has subsided, simple anoscopy helps visualize the exact location of the fissure, as well as any associated papillae or hemorrhoids. Proctoscopy is used to examine higher sections of the rectal canal.
If a fissure is off-midline, multiple, treatment-resistant, or accompanied by warning signs—such as unexplained weight loss or long-standing changes in bowel habits—colonoscopy is necessary to rule out inflammatory bowel disease or more proximal lesions. This distinction is important because not all fissures require colonoscopy, but in atypical cases or in patients over the age of 40, a full colorectal evaluation is recommended.
In patients who are candidates for treatments that alter sphincter tone (such as Botox injection), or when evaluating the cause of preoperative incontinence, anorectal manometry provides measurements of resting and squeeze pressures of the sphincters and helps guide clinical decision-making.
(Step-by-step guide from conservative management to surgical options)
Principle:Management begins with the least invasive and simplest measures. If adequate healing does not occur after a reasonable period (typically 6–8 weeks), or if the fissure becomes chronic, treatment progresses to the next tier of options.

These simple measures lead to improvement in many patients during the acute phase; however, the longer the fissure has been present, the lower the likelihood that it will heal with conservative measures alone.
Studies show that these medications are effective for acute fissures and for some chronic cases; however, their healing rates are lower compared with surgical treatment.
The surgical gold standard
(For patients at risk of incontinence or in whom LIS is not appropriate)
No — many acute fissures heal with dietary fiber, stool softeners, and sitz baths. Only chronic or treatment-resistant fissures require more advanced or invasive interventions.
Botox is a temporary, minimally invasive option with a moderate success rate. LIS offers a higher and more durable healing rate, but carries a slightly greater risk of functional side effects. The choice between the two depends on clinical factors and the patient’s preferences.
Persistent incontinence is not common, but reported rates vary across studies. Pre-operative risk assessment — including childbirth history, endoanal ultrasound (EAUS), and anorectal manometry — is essential for minimizing the likelihood of postoperative functional problems.
An anal fissure is a painful tear in the skin of the anal canal, typically accompanied by pain and bright red bleeding. Most fissures improve with dietary changes, stool softeners, and warm sitz baths. If healing does not occur within 6–8 weeks, treatments such as topical medications, Botox injections, or a minor surgical procedure (lateral internal sphincterotomy) may be recommended. The majority of patients recover well with appropriate therapy.Choosing the most suitable treatment requires a thorough examination and consultation with a colorectal surgeon.