
Laser Treatment Center for Anal Conditions
Colorectal Cancer Treatment Center
Descending colon cancer is a tumor that begins in the inner lining of the large intestine in the descending segment (on the left side of the body). It may initially grow without noticeable pain or symptoms, then infiltrate deeper layers of the bowel wall, spread to nearby lymph nodes, or metastasize through the bloodstream to other organs such as the liver or lungs.
Compared with ascending and sigmoid colon cancers, descending colon cancer is less common and accounts for about 5–7% of all colorectal cancer cases. Globally, this cancer typically appears in the sixth and seventh decades of life and is often associated with symptoms such as changes in bowel habits and overt bleeding. In Iran, official statistics rarely report cases by exact location, but available evidence suggests that descending colon cancer has a distribution similar to global patterns and, unlike right-sided colon cancers, is sometimes reported at relatively younger ages.
This process is usually long and stepwise, and understanding it is essential for appreciating the importance of screening:
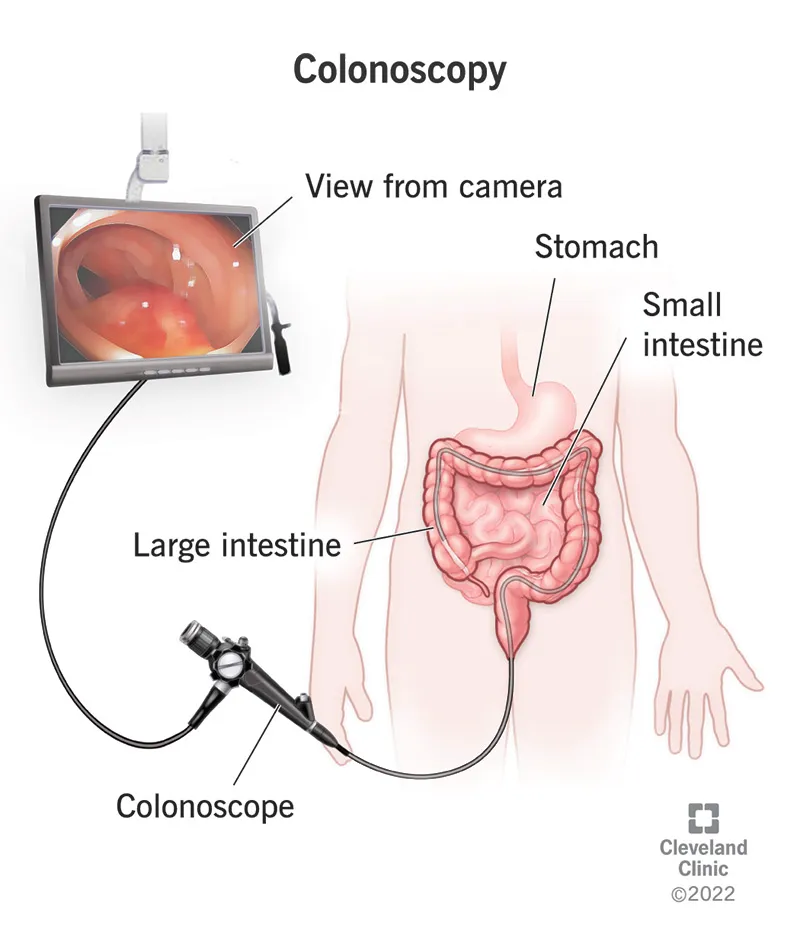
Key point: This sequence typically takes many years; therefore, regular colonoscopy and polyp removal greatly increase the chance of preventing cancer.
I divide the risk factors into two groups: non-modifiable and modifiable, and explain the role of each.
Some early symptoms may be mild or nonspecific; however, the presence of anemia or weight loss should always be taken seriously and warrants thorough evaluation.
Treatment is determined by several factors: the stage of the tumor (its size, depth of invasion, and lymph node status), the patient’s overall condition, and the presence or absence of metastasis.
Neoadjuvant therapy (before surgery): In selected cases, it may be used to shrink the tumor or achieve faster disease control, although its use in colon cancer is less common than in rectal cancer.
Goal: If all liver lesions can be completely removed or locally controlled, and the remaining liver volume after resection is sufficient, a curative treatment approach may be possible. Key considerations include:
Overall patient condition and liver function:The patient must be able to tolerate surgery, and the liver must not be severely impaired.
After 5 years: If everything remains stable, the intensity of follow-up decreases, but annual visits and general health monitoring continue.
Yes. A high-fiber diet, reducing processed meats, maintaining a healthy weight, and staying physically active all help lower the risk and support recovery after treatment.
Not necessarily. In many cases, if the liver lesions are removable or can be locally controlled and the patient is in good overall condition, surgical removal or local treatment of liver metastases can still be pursued with curative intent. This decision is made by a multidisciplinary team.
Usually one year after the operation; if the result is normal, the next exam is done after 3 years, and then every 5 years. However, the schedule may be adjusted depending on previous findings.
There is no absolute guarantee that cancer will “never return,” but evidence shows that a healthy lifestyle reduces the risk of recurrence and improves quality of life.
High fever, sudden and severe abdominal pain, heavy rectal bleeding, persistent nausea and vomiting, or foul-smelling discharge from the surgical incision are warning signs that require urgent medical attention.
Descending colon cancer is a condition that can be diagnosed and, in many cases, effectively treated—especially when detected early. A combination of surgery, chemotherapy when needed, and careful follow-up greatly improves the chances of successful treatment. Positive changes in diet, weight, and physical activity can help reduce the risk of developing or recurring disease and support better treatment outcomes.