
Laser Treatment Center for Anal Conditions
Colorectal Cancer Treatment Center
Uterine and vaginal prolapse refer to the descent of the uterus or vaginal walls into the vaginal canal due to weakened pelvic floor muscles and ligaments. These conditions can lead to symptoms like pelvic pressure, bulging, and sometimes urinary problems. Treatment options range from simple methods (such as diet, Kegel exercises, and pessaries) to minimally invasive or open surgeries. Most women experience significant improvement with proper care and the right treatment approach. The decision regarding treatment is based on the severity of symptoms, patient preferences, and a thorough examination.
Uterine and vaginal prolapse are more common in women, especially after the age of forty and fifty, and the prevalence increases with age. Estimates suggest that a significant percentage of middle-aged to elderly women show degrees of prolapse upon examination, although not all are symptomatic. A history of vaginal childbirth, higher body weight, chronic constipation, and genetic conditions leading to weak connective tissue increase the prevalence of prolapse.
The causes and predisposing factors can be divided into several groups:
Note: The cause is typically not a single factor; it is usually a combination of childbirth-related damage and gradual factors that lead to prolapse.
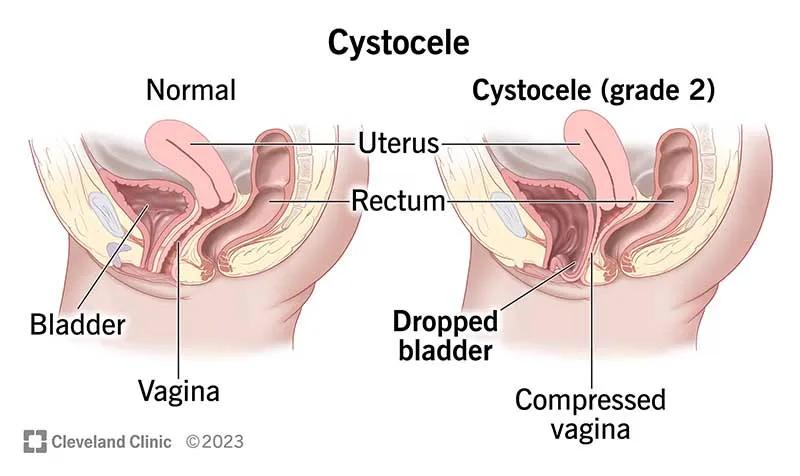
The vagina and uterus are supported by a network of supportive fasciae (such as paravaginal fascia) and pelvic floor muscles. When these fasciae become weak or torn, or when the pelvic floor muscles are paralyzed or stretched, the intra-abdominal pressure is no longer evenly distributed. Over time, this causes the walls to become lax and protrude. Types of prolapse, based on the dominant location, include anterior prolapse (cystocele), apical prolapse (vaginal or uterine vault prolapse), and posterior prolapse (rectocele), which are often seen together.
Questions the doctor may ask: Duration and intensity of pain, bowel movement sequence, constipation or diarrhea, history of pregnancy/childbirth, use of anticoagulant medications, warning signs (weight loss, fever, heavy bleeding, systemic symptoms). This information is crucial for determining the need for further investigations.
A thorough examination of the skin around the anus typically provides the diagnosis; fissures are most commonly seen along the posterior midline. Digital rectal examination (DRE) is only performed if the patient can tolerate it or under anesthesia.
After initial pain relief, simple anoscopy helps visualize the position of the fissure, associated papilla, or hemorrhoids. Proctoscopy is used to examine higher areas.
If the fissure is: non-midline, multifocal, resistant to treatment, or accompanied by warning signs (weight loss, long-term changes in bowel habits) → colonoscopy is essential to rule out inflammatory bowel disease or higher lesions. This is important because not all fissures require colonoscopy, but in unusual cases or for patients over 40, a full colon evaluation is recommended.
In patients who are to undergo treatments that stimulate tone (such as Botox) or who need an evaluation of incontinence before surgery, anorectal manometry will assess resting pressure and sphincter contraction, aiding in decision-making.
These methods can be particularly beneficial in mild to moderate cases and for maintaining quality of life.
No. If the symptoms are mild, conservative options like pessary use and pelvic floor exercises are suitable. Surgery is recommended when symptoms affect daily life or sexual relations, or if non-surgical treatments are not effective.
A pessary is a silicone or plastic device that is inserted into the vagina to provide support. The doctor will measure the appropriate size and provide instructions for replacement or regular follow-up visits for care.
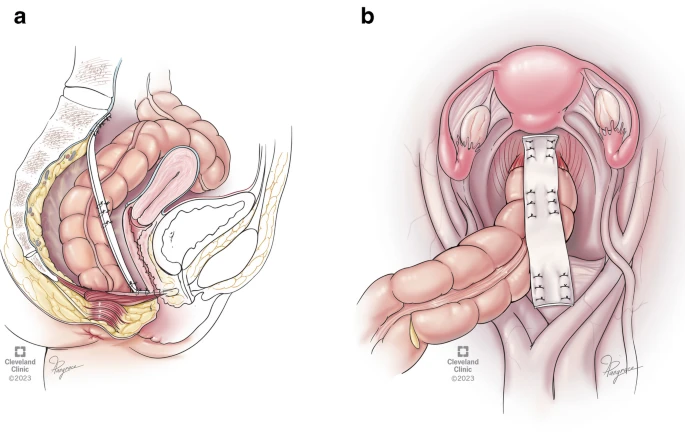
Laparoscopy or robotic surgery offers similar oncological outcomes, less pain, faster recovery, and better nerve protection. These techniques are especially recommended for abdominal repairs or sacrocolpopexy in specialized centers.
Initial Post-Operative Care Relative Rest: Take it easy initially, avoiding prolonged straining and heavy lifting for a few weeks. Pelvic Floor Physiotherapy: Recommended if advised by your doctor to aid recovery. Follow-Up Appointments: Attend scheduled follow-up visits as instructed by your healthcare provider to monitor your recovery.
Uterine and vaginal prolapse refers to the descent of pelvic structures, which can cause feelings of pressure, urinary problems, and discomfort during intercourse. Treatment options vary from exercises and pessary use to vaginal or abdominal surgeries (laparoscopic/robotic). The best treatment approach is chosen based on the severity of symptoms, your preference for preserving the uterus, and examination and imaging findings. In specialized centers, minimally invasive methods performed by experienced surgeons typically yield more durable results.