
Laser Treatment Center for Anal Conditions
Colorectal Cancer Treatment Center
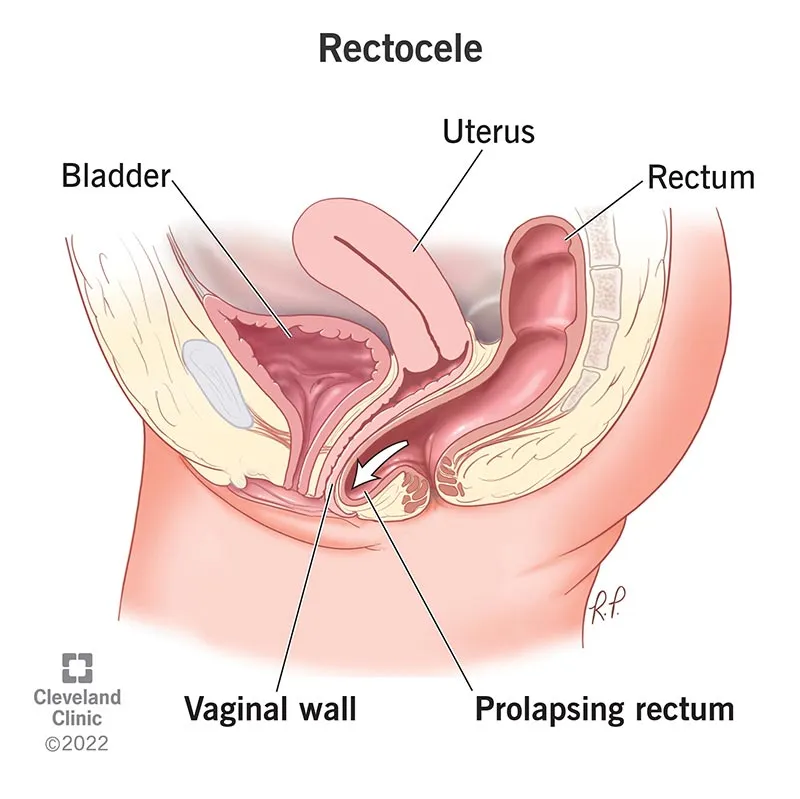
A rectocele occurs when the wall separating the rectum and the vagina (the rectovaginal septum, or the “posterior vaginal wall”) becomes weak and lax, allowing a portion of the rectum to bulge into the vagina. This condition is exclusively a female problem—men do not naturally have a vagina and therefore typically do not develop a rectocele.
Two key processes broadly lead to the development of a rectocele: repeated increases in intra-abdominal pressure and alteration or damage to the supportive tissues.
Note: The severity of symptoms does not correlate directly with the size of the rectocele; some small rectoceles are highly symptomatic and vice versa.
Kegel exercises (pelvic floor training)
No. If the symptoms are mild, non-surgical measures are often sufficient. Surgery is considered when symptoms are present and conservative methods have not been successful.
Because it provides both functional and anatomical information simultaneously: the depth of the rectocele, intussusception, enteroceles, levator muscle status, and perineal descent — all of these are critical for selecting the appropriate surgical method.
Typically, results can be seen within 6–12 weeks with regular practice. If there is no progress after this period, a physiotherapy evaluation is necessary.
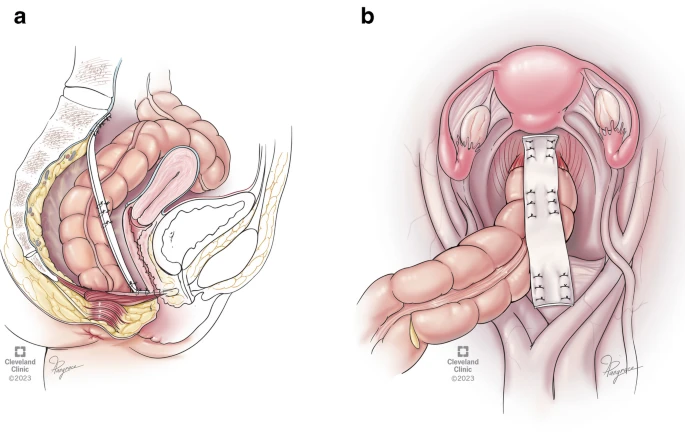
In many cases (especially for large rectoceles or those with multi-organ prolapse), laparoscopy has clear advantages: less pain, quicker recovery, and better nerve preservation. However, the “best” method always depends on the patient’s condition and the surgeon’s experience.
Yes, if the patient has not had a recent colonoscopy, is over 50 years old, or has warning signs, it is necessary to rule out any lesions that may affect the treatment plan.
Rectocele refers to the bulging of the front of the rectum into the vagina due to weakness in the supportive wall. Many patients improve with simple treatments like constipation management and pelvic floor exercises. In symptomatic cases, or when the patient needs “manual assistance” for bowel movements, surgical treatment is considered. Dynamic MRI and defecography help in precisely identifying the problem, allowing the best approach (often laparoscopic in complex cases) to be chosen. Team-based decision-making and surgery performed by an experienced center and surgeon yield the best outcomes.