
Laser Treatment Center for Anal Conditions
Colorectal Cancer Treatment Center
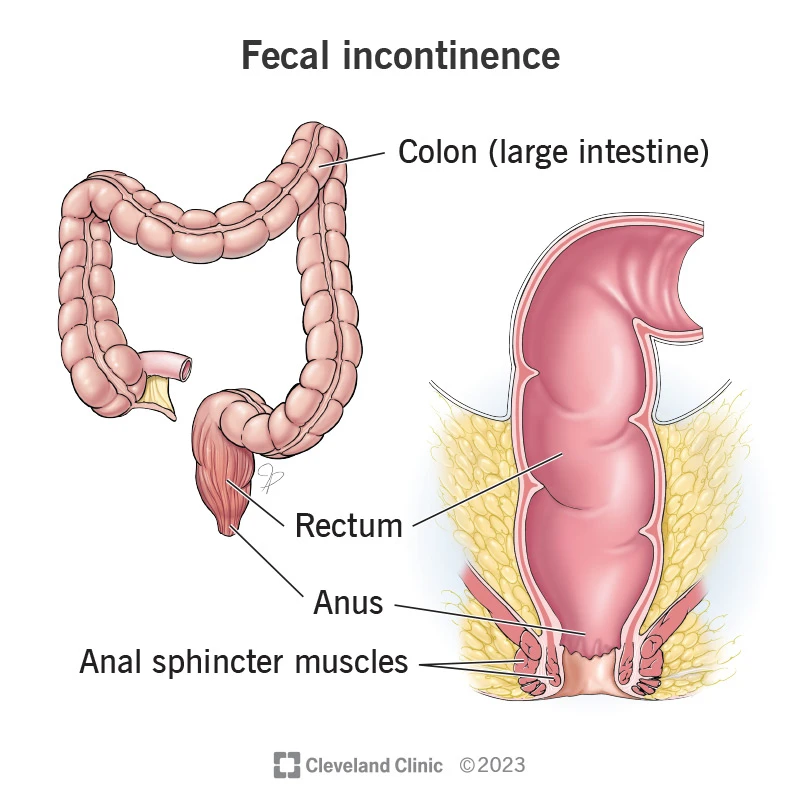
Fecal incontinence is the inability to control the passage of gas, mucus, or stool (liquid or solid) in a way that causes problems for the patient — ranging from minor soiling of underwear to complete loss of control.
Beyond its physical impact, it carries a significant psychological and social burden.
The goal of treatment is to restore comfort and improve quality of life.
This condition is more common than it appears, as many patients feel embarrassed and do not report their symptoms.
Many mild cases go unreported.
Fecal incontinence is often multifactorial.
During vaginal childbirth, the baby’s head passes through the birth canal and may exert pressure on the perineal tissues and the muscular ring surrounding the anus. In some cases, this leads to partial or complete tears of the external or internal anal sphincter. These injuries—known as OASIS (Obstetric Anal Sphincter Injuries)—can vary in severity, and deeper tears result in greater functional impairment. In addition to tearing, prolonged stretching and pressure can damage the pudendal nerve. When this nerve is injured, the neural signals needed for rapid and strong sphincter contraction are disrupted.
Therefore, in many patients, leakage results from a combination of muscular injury and nerve damage.
Removal of tumors, deep hemorrhoidectomies, or surgeries performed close to the anal sphincter can lead to scarring or partial disruption of the sphincter muscle.
Conditions such as advanced diabetes, spinal cord injuries, multiple sclerosis, or stroke can disrupt neural pathways and reduce the ability to maintain continence.
Crohn’s disease and complex fistulas can damage the supporting structures of the anorectal region and impair continence.
Radiation to the pelvic area can injure tissues and nerves, leading to impaired sphincter function and fecal incontinence.
Very loose stool makes continence difficult, while extremely hard stool can lead to leakage of liquid around the impacted stool.
With advancing age, muscle tone and rectal sensation gradually decrease, which can contribute to impaired continence.
Prevention has two aspects: during childbirth and through lifestyle measures.
The anal canal functions through two main sphincters. The internal anal sphincter (a smooth muscle) provides resting pressure, while the external anal sphincter (a skeletal muscle) enables voluntary contraction when needed. The pelvic floor muscles and supporting tissues maintain the rectoanal angle, which is crucial for continence. The pudendal nerve (arising from S2–S4) supplies sensation and motor control to these muscles. Damage to any of these components—muscle, supporting tissues, nerve supply, or any combination—can lead to leakage or urgency. Understanding which specific structure is impaired helps determine the most effective treatment approach.
Patients may experience soiling of underwear, passage of gas accompanied by leakage of liquid stool, an inability to reach the toilet in time (urgency), or loss of stool during activities such as coughing or lifting heavy objects.
Because many individuals feel embarrassed, they may delay seeking medical help; therefore, clinicians should ask targeted questions about childbirth history, previous surgeries, the nature of symptoms, and their impact on daily life. Questionnaires such as the Wexner score help quantify the severity of incontinence and are useful for monitoring treatment progress.
A detailed history is essential (onset of symptoms, relation to childbirth or surgery, type and frequency of leakage, stool consistency, and impact on daily life).
A digital rectal examination is the foundation of diagnosis: it assesses resting and squeeze tone of the anal sphincters and can detect masses, ulcers, or discharge.
This test provides a direct image of the anal sphincter rings.
A probe is inserted into the anal canal to produce cross-sectional and three-dimensional views of the internal and external sphincters and surrounding tissues.
EAUS is the best method for identifying sphincter tears, determining the size and location of defects, and planning surgery.
The procedure usually causes only mild discomfort and requires no complex preparation.
A sensor catheter is placed inside the anal canal to measure resting pressure, squeeze pressure, and responses in different situations.
These measurements help identify whether the problem is primarily low resting pressure (internal sphincter dysfunction) or weak voluntary contraction (external sphincter or nerve dysfunction).
Manometry is crucial for selecting the appropriate treatment.
When nerve injury is suspected, EMG and pudendal nerve terminal motor latency (PNTML) testing provide valuable information. These tests help determine whether muscle repair alone is likely to be effective or if significant nerve damage is present.
These functional imaging studies evaluate defecation in real time and identify conditions such as rectal prolapse, rectocele, intussusception, or outlet obstruction.
Dynamic MRI has the added advantage of excellent soft-tissue visualization and shows the relationship between the rectum and other pelvic organs.
If bleeding or a history of inflammatory disease is present, colonoscopy is necessary to rule out underlying pathology.
Combining these findings—anatomic imaging + functional data + clinical examination—guides the treatment plan.Interpretation and decision-making should always be performed by an experienced colorectal surgeon.
(Step-by-Step Guide)
The goal is to achieve an ideal stool consistency (Bristol types 3–4). For loose stools: use soluble fiber and antidiarrheal medications (such as loperamide) under medical supervision. For constipation or “leakage around hard stool”: use stool softeners and treat impaction as needed. Supportive measures include protective pads, skin-barrier creams, and education about toilet timing and proper defecation posture.
Specialized pelvic floor physiotherapy combined with biofeedback can help restore muscle coordination and strength, especially in patients whose primary issue is functional dysfunction rather than anatomical defects.
The course of therapy typically lasts from several weeks to a few months and should be attempted before considering surgical options.
Bulking agent injections:
Submucosal injection of materials such as hyaluronic acid or specialized polymers is used to thicken the anal canal walls and improve closure.
These procedures are typically performed on an outpatient basis, and their effects may be temporary or long-lasting.
The choice of material and the technique should be determined by an experienced specialist team.
Possible complications include pain, inflammation, or migration of the injected material.
Sacral Nerve Stimulation (SNS) A short test phase is performed first; if the patient shows significant improvement during this trial period, a permanent device is implanted. SNS is a highly effective option with durable long-term results for patients who have not responded to conservative care and physiotherapy, and whose functional testing suggests a good likelihood of response. Implantation and follow-up of the device must be carried out in experienced centers and under the supervision of a colorectal surgeon.
Key points: This operation should be performed only by a specialist colorectal surgeon.
When simple sphincter repair is unsuccessful or when there is extensive nerve damage, additional options may be considered, including: Graciloplasty Artificial anal sphincter implantation And, as a last resort, stoma creation (colostomy) These procedures are complex, carry potential complications, and require close long-term follow-up. They should only be performed in highly specialized centers by experienced surgeons.
Complete sphincter tears should be repaired and carefully followed.
The final decision depends on the severity of the injury and the patient’s symptoms, and should be made in consultation with a colorectal surgeon.
Early repair generally provides better outcomes when performed by an experienced team.
However, if primary repair was not performed, a thorough evaluation and elective reconstruction under the care of a colorectal surgeon can still be beneficial.
The trial phase usually causes only mild discomfort.
If the response is positive, a permanent device is implanted, and it can be adjusted to optimize comfort and effectiveness.
Some materials have long-lasting effects, but repeat treatments may still be necessary.
The choice of material and the expectations for durability should be clearly discussed with the specialist.
Fecal incontinence is a condition that can be properly diagnosed and, in many cases, effectively treated. Management typically begins with dietary adjustments, stool optimization, and pelvic floor exercises. If these measures are not sufficient, detailed functional tests and imaging studies are performed. Based on the results, treatment may include bulking agent injections, sacral nerve stimulation, or reconstructive surgery. All surgical or reconstructive decisions should be made and performed by a specialized colorectal surgeon to ensure the highest chance of improvement with the lowest risk of complications.