
Laser Treatment Center for Anal Conditions
Colorectal Cancer Treatment Center
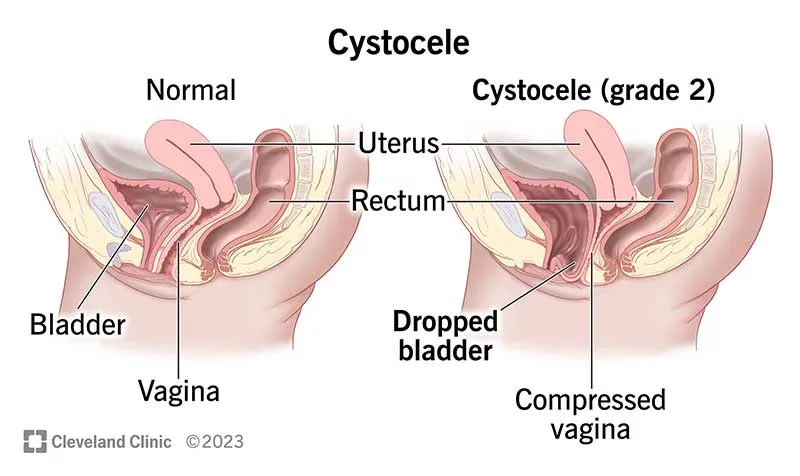
Cystocele refers to the downward displacement or prolapse of the anterior wall of the vagina, causing a portion of the bladder to bulge or herniate into the vaginal wall. In simple terms, the wall that supports the bladder weakens, and the bladder moves from its natural position toward the vagina.
Cystocele and pelvic organ prolapse are common in women and tend to increase with age. Depending on the study, signs of prolapse are observed in a significant percentage of women when examined, but not all cases are symptomatic. This means many cases are only detected during an examination, with the patient not experiencing pain or discomfort. Demographic factors and pregnancy/childbirth play an important role in the prevalence of this condition.
Cystocele is the result of weakness or damage to the tissues and supporting structures of the bladder and vagina. The main causes include:
In a healthy state, a strong layer of muscle and connective tissue (pubocervical fascia) supports the bladder within the pelvic cavity. When this fascia or the pelvic floor muscles become weakened or torn:
This process takes years and is a combination of acute damage (e.g., from difficult childbirth) and gradual factors (such as constipation, obesity, and menopause).
Symptoms can range from mild to severe. The most common complaints include:
The severity of symptoms does not necessarily correlate with the size of the protrusion; some women with small prolapses experience significant issues, while others with larger prolapses may have few symptoms.
Questions should focus on the onset of symptoms, association with pregnancies, constipation, history of pelvic surgery, medications, and impact on quality of life.
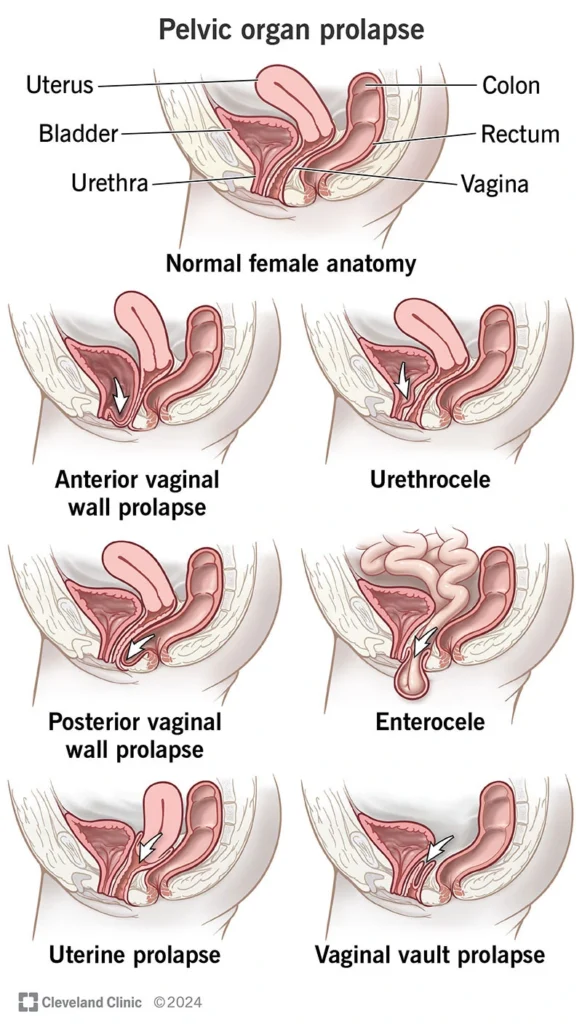
The doctor will ask you to bear down (Valsalva maneuver) to observe the prolapse. A vaginal internal examination is performed to visualize the location of the bulge and assess any accompanying elements (e.g., simultaneous rectocele/uterine prolapse).
POP-Q is a set of simple measurements at defined vaginal points that helps quantify the severity of prolapse; this standard is useful in reporting and comparing surgical outcomes. (Although the name is technical, its purpose is to precisely document the location and severity of the prolapse to improve treatment planning.)
If urinary problems are present, urodynamics may be needed to assess the type of incontinence or outlet obstruction (especially when surgery is planned, as some surgeries may worsen or improve urinary symptoms).
Clinical diagnosis is usually sufficient, but in complex cases or when multiple organs are prolapsing or there are unusual symptoms, imaging can be helpful.
Important Notes:Correct technique is essential; some women may mistakenly contract abdominal or buttock muscles instead of the pelvic floor. It is recommended to have initial sessions with a pelvic floor physiotherapist to personalize the technique and plan. Guided programs have shown to be more effective.
Care Tips: The pessary should be fitted by a doctor or nurse (size and type selection). Patients or the team are trained to change, clean, and care for the pessary. Regular check-ups are required (e.g., every 3–6 months or as instructed). If pain, bleeding, or foul discharge occurs, immediate consultation is needed.
Note: Decision-making should be shared with the patient; the priority is an effective, minimally invasive approach suited to the individual’s condition.
No — if the symptoms are mild, you can start with pelvic floor exercises, pessary use, or conservative care first. Surgery is typically considered if these methods do not provide relief or if symptoms become severe.
As if you are trying to stop the flow of urine for a few seconds: Contract the muscles, hold for 3–5 seconds, then relax; repeat 8–12 times per session, 3 times a day. To ensure proper technique, consult with a pelvic floor physiotherapist.
The doctor will select the appropriate size and insert it in the office. The procedure is usually painless or causes only minimal discomfort. You will need to learn how to maintain the pessary and when to replace it, with regular follow-up visits to ensure proper fit and function.
Yes, having a cystocele does not necessarily prevent pregnancy or childbirth. However, it is important to consult with your healthcare provider for proper management during pregnancy and delivery. They may recommend certain precautions or treatments to prevent further weakening of pelvic structures during childbirth.
It depends on the type and severity of the prolapse, the patient’s age, preferences, and the experience of the team. Vaginal repair is suitable for more localized cases; however, for multi-compartment prolapse or when long-term durability is required, laparoscopy/sacrocolpopexy may offer more durable benefits. The final choice is made through a team discussion.
Cystocele refers to the prolapse of the bladder into the vagina, which causes feelings of pressure, a bulge inside the vagina, and sometimes urinary problems. Treatment ranges from the simplest methods (diet, Kegel exercises, pessaries) to minimally invasive or open surgeries. Most women experience significant improvement with proper care and the right choice of treatment. The decision regarding treatment is made based on the severity of symptoms, your preferences, and a thorough examination.