
Laser Treatment Center for Anal Conditions
Colorectal Cancer Treatment Center
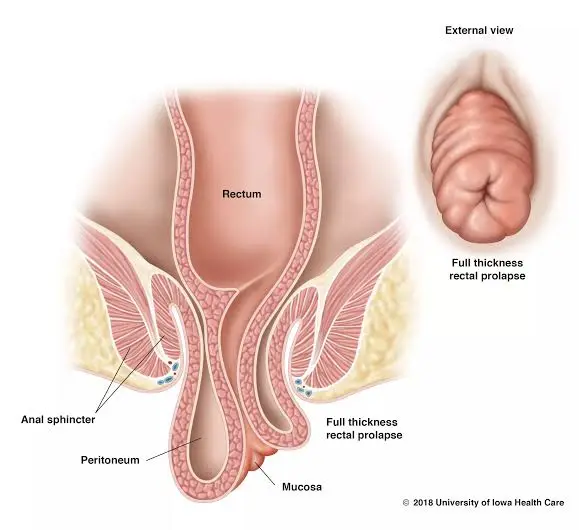
“Perineal descent” means the excessive lowering or falling of parts of the pelvic floor (perineum) and its supporting structures relative to their normal position. When the patient strains (such as during defecation), the terminal part of the gastrointestinal tract (anorectal) and the perineal area (the area between the anus and the genitals) descend excessively — this phenomenon may cause problems such as defecation problems (feeling of incomplete evacuation, straining), leakage of stool or gas, a feeling of heaviness or bulge in the pelvic area, and sometimes disrupt sexual relations or urinary function.
If the pelvic diaphragm or the supportive structures of the pelvic floor are loose or damaged, they allow the rectum and perineum to descend or the contents inside the canal to shift.
These structures and the way they support determine why some individuals experience descent and why symptoms may worsen with straining.
Perineal descent is observed at almost any age, but it is more common in middle-aged and elderly individuals.
It is more prevalent in women (particularly those who have had multiple deliveries, especially vaginal deliveries with perineal injury), though men can also be affected (for example, after prostate surgery or due to neurological injury). Therefore, we should not say it only affects women—although prevalence is higher in women. Other factors that increase prevalence include: chronic constipation and prolonged straining, obesity, chronic cough, diseases that cause weakness of connective tissue, and certain neurological injuries.
The causes are typically multifactorial and complex; the most important mechanisms include:
Difficult childbirth, prolonged perineal stretching, or sphincter tears and/or levator avulsion injuries can weaken the supportive structures. This is one of the most common causes in women.
Repetitive straining during defecation causes prolonged pressure on the supporting structures; over time, the tissues become stretched and weakened, leading to descent.
Nerve damage (such as pudendal nerve injury) resulting from surgery or trauma can lead to impaired muscular function.
Connective tissue disorders (such as related syndromes), obesity, and aging that reduce the quality of connective tissue.
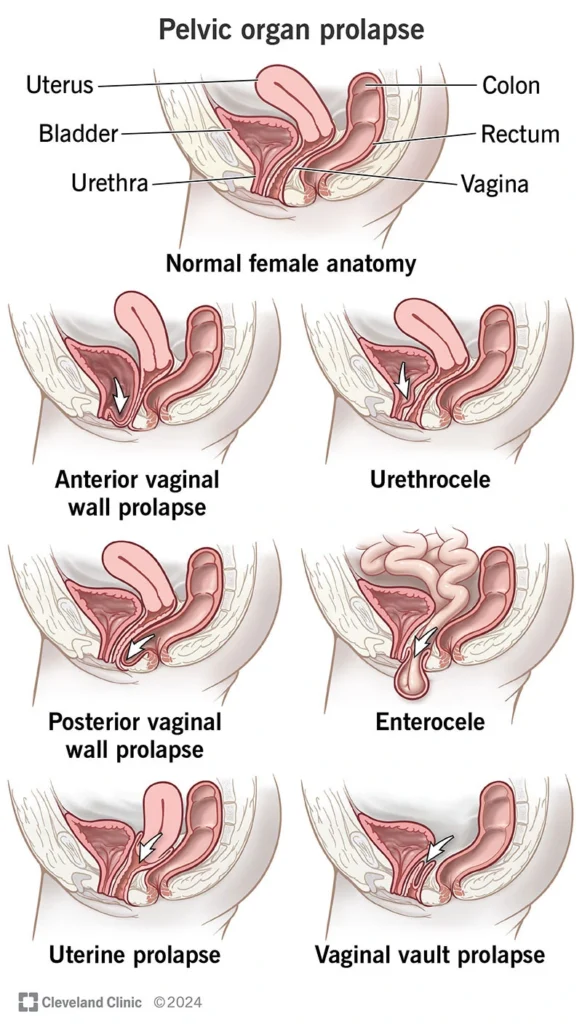
Perineal descent often occurs concurrently with rectocele, cystocele, or uterine prolapse; all of these conditions can coexist and complicate the clinical picture.
Repetitive pressure and/or direct injury → Supportive tissues (ligaments, fascia, levator muscles) gradually stretch and weaken.
Symptoms are varied and multiple symptoms may be present simultaneously:
The severity of symptoms varies from mild discomfort to severe functional impairment.
The diagnosis is a combination of history, physical examination, and functional imaging. I’ve explained what the patient should expect in each section.
A detailed pelvic examination in women includes evaluation of all three pelvic floor compartments (anterior/middle/posterior) to document any associated cystocele or rectocele.
These tests help determine whether sphincter repair is needed and which surgical approach is more appropriate.
Treatment Goal: To reduce symptoms, restore defecatory function, protect the sphincter, and improve quality of life. Treatment is typically staged and selected based on symptom severity, imaging findings, and the patient’s general condition.
If the patient does not respond after a reasonable period (e.g., several months) of conservative treatment and imaging shows significant descent or structural abnormalities, we proceed to interventional options.
In some cases, along with physical therapy, use of a pessary for vaginal/perineal support in women can reduce symptoms (temporary or for patients who are not surgical candidates). This approach is primarily for anterior or middle pelvic floor disorders but may sometimes help reduce the feeling of heaviness.
Surgical decision-making should be multidisciplinary and based on detailed imaging (especially dynamic MRI).
For high-risk surgical patients (e.g., elderly patients with comorbidities), perineal approaches such as Altemeier or Delorme may be chosen. These are less invasive but have a higher recurrence rate in the long term.
Laparoscopy/robotics is generally preferred when the center and surgeon have experience: smaller incisions, less pain, faster recovery, and most importantly, magnification and better visualization for pelvic nerve preservation. These advantages are particularly important in rectal surgery and correction of descent because the pelvic space is small and sensitive.
Important Note: No surgical procedure is “one-size-fits-all.” The choice between abdominal or perineal approach, use of mesh or mesh-free, and need for sigmoid resection are all decided based on imaging findings, sphincter function, and patient goals (anal preservation or not). This decision should be made in a multidisciplinary meeting (colorectal surgeon + radiologist + pelvic floor physiotherapist + gynecologist/urologist if needed).
The colorectal surgeon plays a central role in decision-making, performing the procedure, and long-term follow-up.
No. Many patients improve with diet modification, laxatives, and physical therapy/biofeedback. Surgery is considered when symptoms are severe or imaging shows significant descent.
Often yes; especially if surgery is planned. MRI provides detailed anatomical information and shows the proximity of tumors/descent to surrounding structures, helping to select the best surgical approach.
Many patients experience significant improvement, but some functional changes (such as slight changes in defecation patterns or the need for further exercises) may persist. The treatment team clearly discusses expectations before surgery.
For many patients with functional defecation disorders (especially dyssynergia), biofeedback and physical therapy yield very good results and often prevent surgery or improve post-operative function.
Perineal descent refers to the abnormal downward movement of the supporting structures of the rectum and perineum, which can cause recurrent straining, a feeling of incomplete evacuation, incontinence, or a sensation of heaviness. Diagnosis involves physical examination, defecography, and especially dynamic MRI. Many patients improve with dietary modifications, constipation treatment, and physical therapy — particularly biofeedback; if these methods are insufficient, targeted surgery (often laparoscopic/robotic and sometimes perineal) is performed by a colorectal surgeon. Treatment decisions should be multidisciplinary and based on detailed imaging.