
Laser Treatment Center for Anal Conditions
Colorectal Cancer Treatment Center

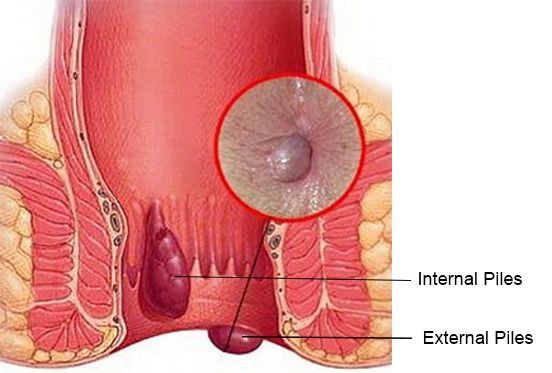
Hemorrhoids occur when the hemorrhoidal cushions—clusters of veins and supporting tissue within the anal canal—become dilated, enlarged, or prolapsed, leading to symptoms.
Under normal circumstances, these cushions help maintain closure of the anal opening; however, when their shape or position changes, they may cause bleeding, pain, or a noticeable lump.
Hemorrhoids are very common, and many adults experience hemorrhoid-like symptoms at least once during their lifetime.
Prevalence increases with age and is also higher during pregnancy.Contributing factors include chronic constipation and straining during bowel movements, prolonged sitting, obesity, pregnancy, chronic coughing, and certain medical conditions—such as liver insufficiency—that elevate venous pressure.
Patients may report one or more of the following symptoms:
Symptoms such as persistent changes in bowel habits, unexplained weight loss, or significant bleeding require further evaluation and may warrant a colonoscopy.
History: Assessment includes questions about the pattern of bleeding, constipation or diarrhea, duration of symptoms, pregnancy, use of anticoagulant medications, family history, and the impact of symptoms on quality of life.
Physical examination: Inspection of the anal region both at rest and during a Valsalva maneuver (straining) to assess for prolapse; digital rectal examination (DRE) to evaluate sphincter tone and to exclude the presence of a significant mass.
Internal hemorrhoids are classified into four grades based on the degree of prolapse, providing a framework for choosing the most appropriate treatment.
The grading system describes how far the tissue protrudes, and whether it reduces spontaneously or requires manual assistance.
It also identifies cases that are irreducible or complicated by secondary inflammation.
This classification is essential for selecting between conservative therapy, office-based procedures, and surgical options.
Before any invasive intervention is considered, constipation correction and conservative treatments are initiated.
These measures are effective for Grade I hemorrhoids and for some Grade II cases, and they form the foundation of initial treatment.

In selected cases—particularly when coexisting colorectal lesions or pelvic procedures also require treatment—laparoscopic or minimally invasive approaches may offer smaller incisions, reduced postoperative pain, and a faster return to normal activity.The choice of technique should be individualized based on the grade of hemorrhoids, the patient’s anatomy, their expectations, and the surgeon’s expertise.
If the patient presents within approximately 72 hours of symptom onset and the thrombosis is evident, evacuation of the clot under local anesthesia typically provides immediate pain relief.
In later presentations or when the thrombosis is older, supportive management may be sufficient.
Common and clinically significant complications include postoperative bleeding or bleeding when the ligation band detaches, pain and discomfort after the procedure, and rare local infections.
In uncommon cases, injury to the sphincter may occur, which can result in some degree of incontinence.
Certain techniques—such as stapled hemorrhoidopexy—have been associated with rare complications including mucosal necrosis or significant bleeding.
Additionally, when a large volume of tissue is removed, there is a risk of developing anal canal stenosis.
The surgeon’s responsibilities include conducting a thorough evaluation of the patient and determining the most appropriate treatment option based on the severity of disease and the patient’s overall condition.
They perform procedures with the aim of preserving sphincter function and minimizing complications.
Preoperative counseling is provided to explain expected outcomes and potential risks, and regular postoperative follow-up is essential to manage complications or recurrence.
Exact figures vary depending on the treatment center and patient selection, and a specialized consultation is essential for determining the most appropriate approach.
Generally, no. Hemorrhoids are usually not dangerous; however, recurrent bleeding, severe pain, or the presence of warning signs—such as unexplained weight loss or persistent changes in bowel habits—warrant further medical evaluation.
If you experience persistent bleeding, severe pain, fever, or any unusual symptoms.
Most conservative measures—such as increasing fiber intake, using stool softeners, and taking sitz baths—are safe and effective during pregnancy.
Invasive procedures are generally deferred until after delivery, unless symptoms are significantly troublesome.
It depends on the type of procedure. Conventional hemorrhoidectomy is typically associated with more postoperative pain, whereas techniques such as stapled hemorrhoidopexy or Doppler-guided artery ligation generally cause less discomfort.
Yes, recurrence is possible. Improving diet and bowel habits—such as increasing fiber intake, ensuring adequate hydration, and avoiding straining—plays an important role in reducing the risk of relapse.
Hemorrhoids are a common condition that occur when the vascular cushions inside the anal canal become dilated or prolapsed, often leading to bright red bleeding, a noticeable lump, pain, or itching.
Diagnosis is based on medical history and physical examination, and in cases with concerning features—such as persistent bleeding or long-standing changes in bowel habits—additional evaluation with anoscopy or colonoscopy may be required. Treatment follows a stepwise approach: dietary modification and increased fiber intake, stool softeners, and local care form the foundation of management.
When intervention is needed, minimally invasive office-based procedures or surgical options may be considered.In our practice, many external hemorrhoids and selected internal cushions can be treated or corrected in the office using CO₂ laser under local anesthesia, typically providing a shorter recovery period and fewer complications compared with operating-room surgery.
More complex cases or extensive prolapse may require open surgery or alternative techniques. The choice of treatment should be individualized, based on the grade of the hemorrhoids, the patient’s overall condition, and personal preference.
A consultation with a colorectal surgeon is the best way to determine the most appropriate management plan.