
Laser Treatment Center for Anal Conditions
Colorectal Cancer Treatment Center
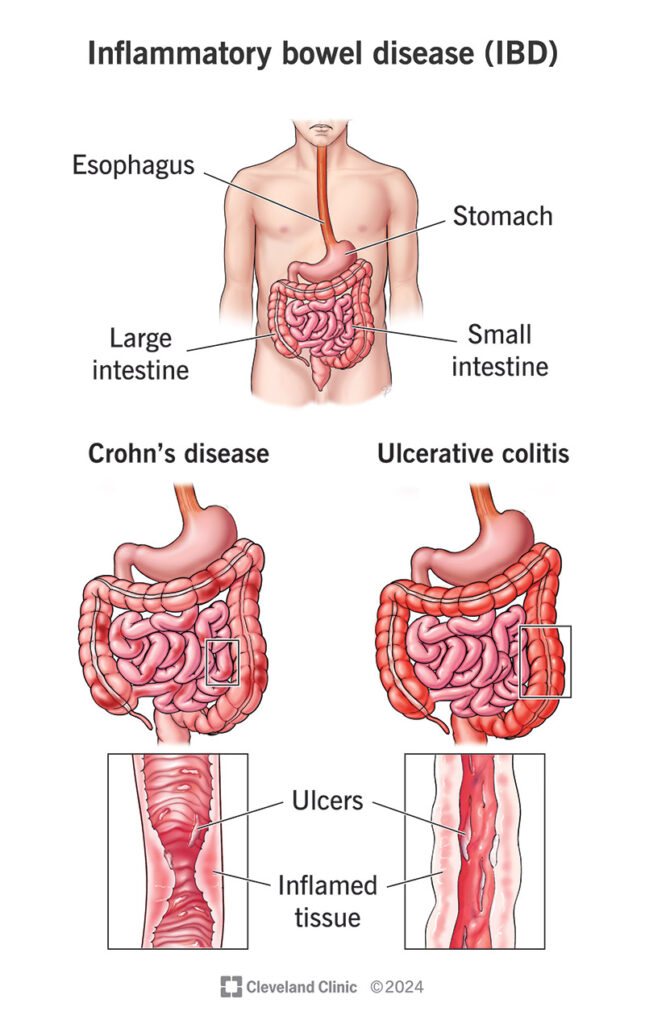
Crohn’s disease is a chronic inflammatory disorder of the gastrointestinal tract, capable of affecting any segment from the mouth to the anus. However, it most commonly involves the small intestine (particularly the ileum) and the large intestine. In Crohn’s disease, inflammation typically appears in a “patchy” distribution and extends through the full thickness of the bowel wall (known as transmural inflammation). This characteristic can lead to deep ulceration, fistula formation, and intestinal strictures.
The exact cause of Crohn’s disease remains unknown; however, several key factors are believed to contribute to its development:
Genetic factors: A family history of inflammatory bowel disease significantly increases an individual’s risk, indicating a strong genetic predisposition
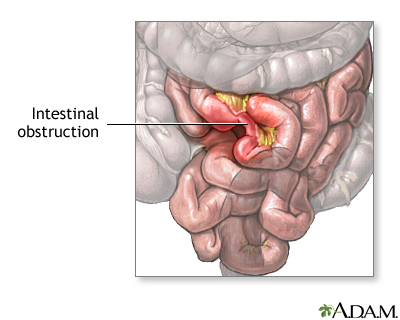
In genetically susceptible individuals, interactions between host genes and the gut microbiome trigger an abnormal localized inflammatory response. This transmural inflammation, characterized by the infiltration of inflammatory cells through all layers of the intestinal wall, leads to the formation of deep ulcerations. Over time, repeated cycles of inflammation and healing promote fibrosis, consisting of collagen deposition and scar tissue formation, which may ultimately result in strictures (narrowing of the intestinal lumen).
When the inflammatory process extends beyond the bowel wall, fistulas may form—abnormal connections between the intestine and the skin or adjacent organs.
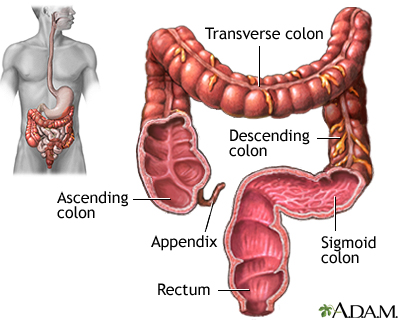
Colonoscopy: Performed to visualize the colonic mucosa and terminal ileum, identify patchy lesions, aphthous ulcers, and the characteristic cobblestone appearance, and to obtain biopsies for microscopic evaluation.
Histologic samples may demonstrate chronic inflammation, epithelioid granulomas in a subset of patients, and other changes characteristic of Crohn’s disease.
(Step-by-step guide)
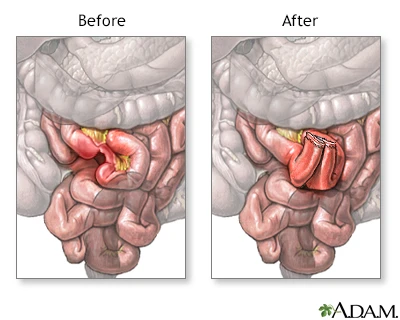
In Crohn’s disease, surgery does not cure the condition, but it plays a crucial role in managing complications. Situations in which a colorectal surgeon becomes involved include:
When selecting a surgical technique, the priority is to preserve as much healthy bowel as possible and to prevent short bowel syndrome, which can occur when excessive lengths of intestine are removed.
Crohn’s disease follows a relapsing–remitting course; however, with modern therapies, many patients experience significantly improved quality of life and a reduction in disease-related complications.
No — Crohn’s disease is a non-infectious inflammatory condition. It arises from a combination of genetic predisposition and an abnormal immune response to gut microbiota, and it cannot be transmitted from one person to another.
Calprotectin is a protein found in white blood cells that increases in the stool when intestinal inflammation is present.
A fecal calprotectin test helps determine whether a patient’s symptoms are due to true intestinal inflammation (as seen in Crohn’s disease) or related to non-inflammatory conditions such as irritable bowel syndrome (IBS).
Immunomodulators are medications that broadly reduce immune system activity to prevent recurrent inflammation.
Biologic therapies act in a more targeted manner: they block specific proteins or inflammatory molecules involved in the immune response. Because of this precision, biologics are highly effective in patients with moderate to severe Crohn’s disease.
Surgery in Crohn’s disease is typically performed to manage complications such as strictures, fistulas, abscesses, perforation, or severe bleeding.
It does not eliminate the underlying disease, and recurrence in other segments of the intestine may still occur.
Therefore, the primary goal of surgery is to address complications and preserve or improve the patient’s quality of life.
The need for surgery varies from patient to patient and depends on the severity, location, and behavior of the disease.
Historically, many individuals with Crohn’s disease required at least one surgical procedure during their lifetime, usually to treat complications such as strictures, abscesses, or fistulas.
With modern medical and biologic therapies, the overall need for surgery has decreased, but it is still possible if complications develop or if the disease does not respond adequately to medication.
Yes. Most women with Crohn’s disease can have successful pregnancies.
The best time to conceive is when the disease is well controlled.
Some medications may need adjustment before or during pregnancy, and your medical team will guide you to ensure both maternal and fetal safety.
Crohn’s disease is a chronic inflammatory condition of the intestines that can cause abdominal pain, diarrhea, weight loss, and, in some cases, complications such as abscesses or fistulas.
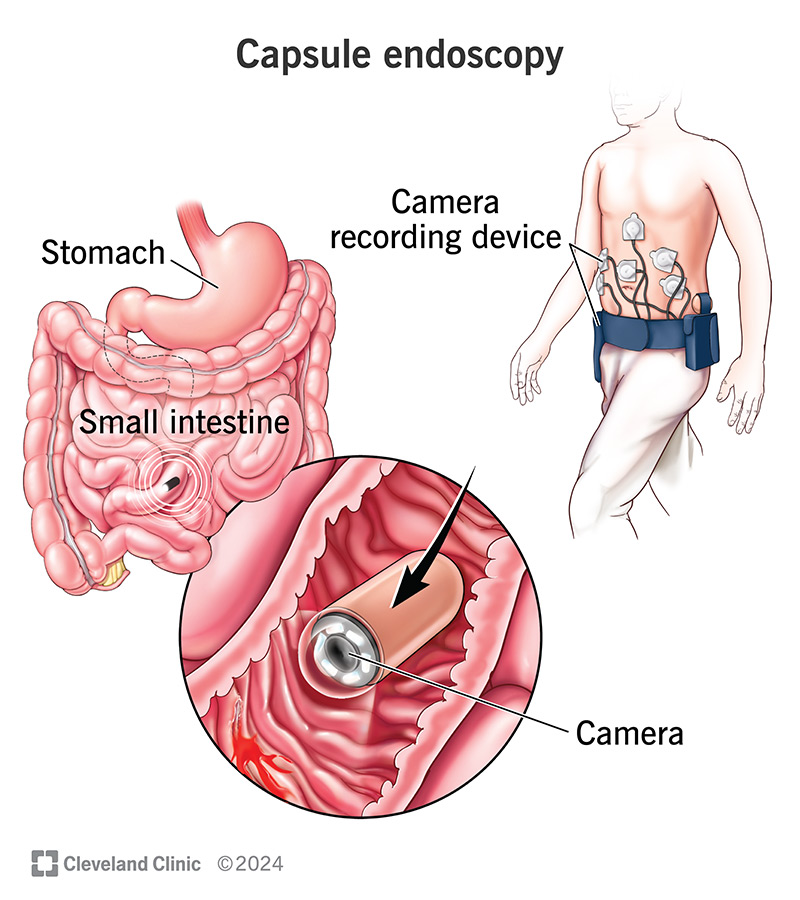
Diagnosis typically involves a combination of blood tests, stool testing (including fecal calprotectin), colonoscopy, and imaging studies such as MRI or CT scans. Treatment focuses on reducing inflammation — using medications ranging from corticosteroids for acute flares to immunomodulators and biologic therapies for long-term control — and surgery may be required if specific complications develop.
The overall goal of treatment is to control inflammation, prevent complications, and maintain a good quality of life.