
Laser Treatment Center for Anal Conditions
Colorectal Cancer Treatment Center
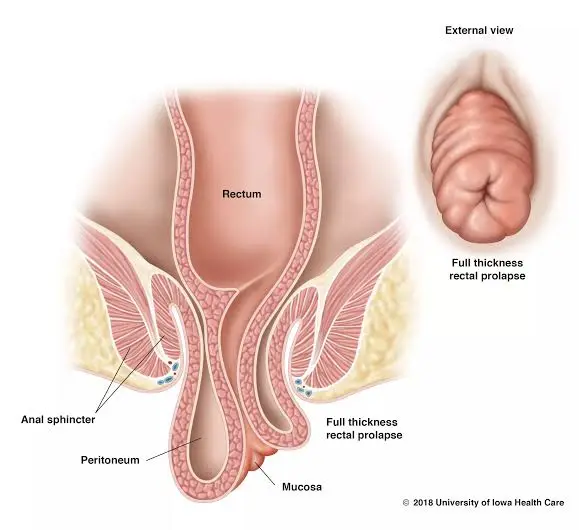
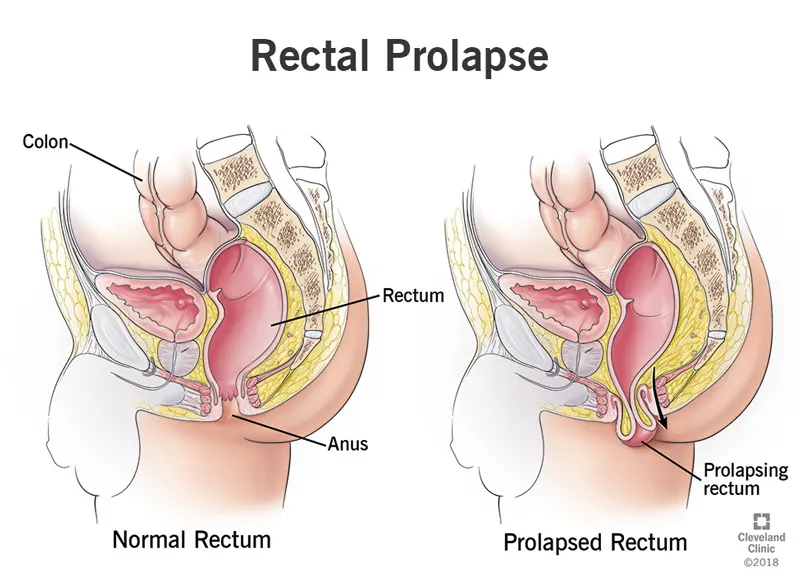
Rectal prolapse refers to the abnormal protrusion of portions of the rectum through the anal canal. This protrusion may involve only the superficial mucosal layer or all layers (full-thickness). Sometimes “internal intussusception” occurs, meaning the rectum telescopes inward but has not yet protruded through the anus. Prolapse can be temporary or may progressively become permanent, affecting quality of life.
The rectum is the final segment of the large intestine, approximately 12-15 cm in length, and is located just before the anus. The rectum’s function is to temporarily store feces and provide conditions for controlled defecation. The rectal wall consists of multiple layers: mucosa (the surface in contact with contents), submucosa, and muscular layers (circular and longitudinal) that maintain movement and tone. Surrounding the rectum are fatty and fascial tissues that anchor it to the pelvis; this supportive structure, when weakened, leads to excessive rectal mobility and makes prolapse development easier.
Important Note: Having one or more risk factors does not necessarily mean that prolapse will occur; these factors only increase the probability.
Severe perineal tears during vaginal delivery, particularly third and fourth degree tears that involve the anal sphincter or rectal mucosa, damage the supportive structures and nerve pathways. Predisposing factors for such tears include prolonged second stage of labor, sudden fetal expulsion, use of forceps or vacuum extraction, large fetus, and multiple deliveries. If these tears are not properly treated or have inadequate repair, the long-term risk of prolapse and incontinence increases.
Repetitive intra-abdominal pressure and repeated straining cause stretching and gradual displacement of the mesorectum and supporting ligaments. Over time, these tissues become “loose” and the rectum moves forward more easily.
Diseases that weaken the nerves controlling the pelvic floor, such as spinal cord lesions or peripheral neuropathies, compromise the supportive tissues and disrupt the rectum’s retaining function.
Previous pelvic surgeries, adhesions, or chronic inflammation can alter the supportive architecture.
Some individuals experience reduced collagen quality and connective tissue due to connective tissue disorders or aging; this leads to decreased ligament strength and significantly increases the risk of prolapse.
Summary of mechanism: The combination of repeated increased pressure, direct injury (such as during childbirth), and changes in supportive tissue quality causes the rectum to gradually displace from its normal position and ultimately protrude.
Patients typically report one or more of the following:
When these symptoms are recurrent or progressive and affect quality of life, it is important to be evaluated promptly.
Examination is performed in both resting and straining positions to visualize the prolapse. Digital examination assesses sphincter tone and checks for any ulcers or inflammation. This examination is the first and most important step.
The physician or radiologist introduces a paste with consistency similar to stool into the rectum. The patient sits on a special chair resembling a toilet, and while the fluoroscopic device records, performs several deep breaths followed by straining to document the actual process of filling and emptying. This film shows when prolapse occurs, whether internal intussusception is present, the depth of the rectocele, and how far the perineum descends. Preparation typically includes simple instructions from the radiology center or a light enema.
MRI performs the same dynamic process without radiation and with greater soft tissue detail. MRI better demonstrates the mesorectum, fascia, relationship with the bladder and vagina, and internal intussusception. For patients with suspicion of multi-compartment involvement or a history of surgery or incontinence, MRI provides essential information for surgical planning.
Endoanal ultrasonography provides direct imaging of the internal and external sphincters and can show tears resulting from childbirth or scarring. Manometry measures resting and squeeze pressures of the sphincters and tells us how the muscular function is. The combination of these data determines whether the patient also needs sphincter repair.
Before surgery, colonoscopy is necessary to rule out concurrent polyps or tumors. If the patient has not previously had a colonoscopy, we typically schedule one.
The decision-making principle is based on the severity of symptoms, the type of prolapse (mucosal or full-thickness), sphincter function, and the patient’s general condition. If the prolapse is mild and without functional impairment, we first try non-surgical treatment. If the prolapse is complete, symptomatic, or has caused ulceration/incontinence, surgery is usually the best approach.
These measures are especially effective in the early stages and for preventing progression.
These methods are usually chosen for elderly patients or those who cannot tolerate abdominal anesthesia. Two main methods:
Abdominal methods typically provide more stable results and lower recurrence rates in younger individuals and those who are suitable for anesthesia. Two important methods:
Summary comparison: Abdominal methods provide more stable functional results, and laparoscopy/robotics can reduce complications and hospital stay duration, but the final selection should be made by a team after evaluating dynamic imaging and the patient’s general condition.
In specific cases of mucosal prolapse or internal intussusception with evacuation disorders, methods like STARR or mucosal stapled rectopexy can be useful, but they are usually insufficient for full-thickness prolapse and patients must be selected very carefully.
Successful and complication-free repair of prolapse requires the surgeon’s experience in laparoscopic/robotic techniques and familiarity with pelvic nerve anatomy.
A good team includes a colorectal surgeon, a radiologist experienced in dynamic MRI/defecography, and a pelvic floor physical therapist. When multi-compartment prolapses exist, collaboration with a gynecologist or urologist is essential.
Final emphasis: Sphincter repair surgeries or complex decisions should be performed by a colorectal surgeon.
Post-discharge care: Soft diet until recovery, stool softeners to prevent straining, sitz baths for local improvement, and pelvic floor physical therapy if needed. The surgeon determines the timing for return to work and strenuous activities.
Prognosis depends on the type of prolapse, treatment method, age, and associated diseases. Generally, surgical correction improves symptoms, and with appropriate method selection and an experienced surgeon, functional outcomes and patient satisfaction are usually good. Abdominal methods typically have lower recurrence rates, but each case must be evaluated individually.
Not if it’s very mild and asymptomatic, but complete and symptomatic prolapse usually requires surgical treatment.
In suitable patients, yes. Laparoscopy or robotic methods provide greater visualization and magnification, along with more precise instruments, which makes protecting pelvic nerves easier, results in less postoperative pain, and allows for a quicker return to daily life. The final choice depends on the patient’s condition and the center’s experience.
If you had a third or fourth degree tear or have had symptoms of leakage or a feeling of protrusion since childbirth, you should definitely see a colorectal surgeon. Early repairs and timely follow-up significantly improve the quality of results.
A high-fiber diet and adequate fluids, stool softeners if needed, avoiding prolonged straining, and treating chronic cough; performing pelvic floor exercises at home is helpful.
Not if it’s very mild and asymptomatic, but complete and symptomatic prolapse usually requires surgical treatment.
Rectal prolapse means the slipping or protrusion of the rectum through the anus. The causes are a combination of obstetric injury, chronic constipation, weakness of supportive tissues, and neurological or tissue factors. Diagnosis is made through examination and dynamic imaging. Simple and low-cost measures such as a high-fiber diet, stool softeners, cough treatment, and pelvic floor exercises can be helpful, but surgery is usually necessary for complete or symptomatic prolapse. If surgery is required, laparoscopic or robotic methods in experienced centers yield good results because they reduce pain, hospital stay, and the risk of nerve injury, and help with a quicker return to daily life. The final decision is made by a multidisciplinary team and a colorectal surgeon.