
Laser Treatment Center for Anal Conditions
Colorectal Cancer Treatment Center
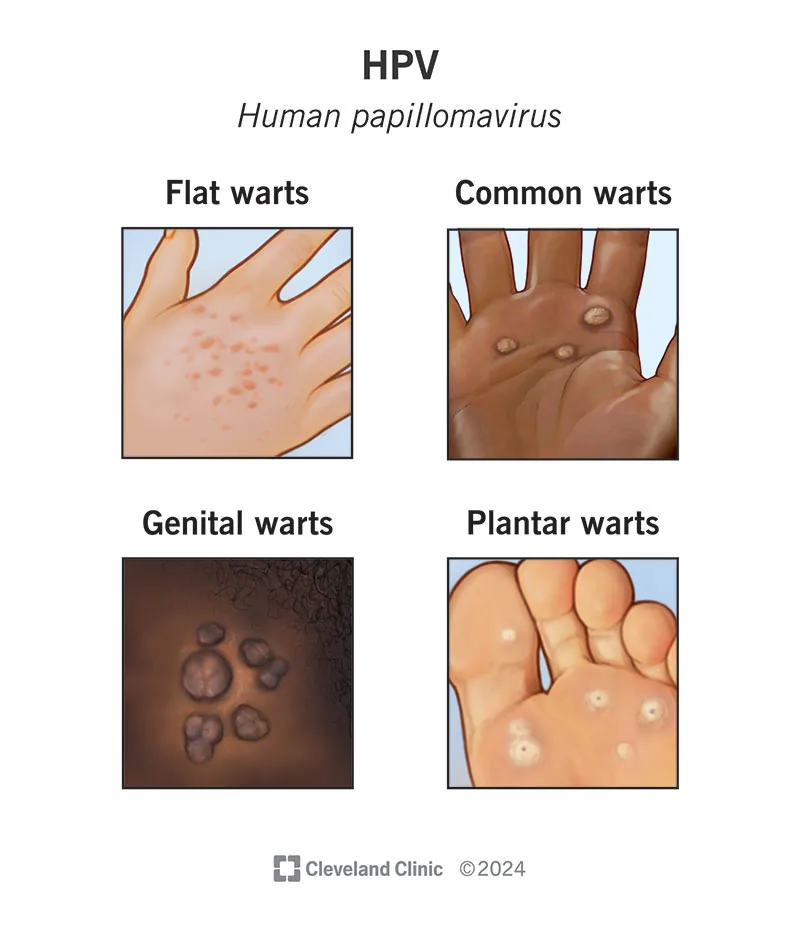
Anal warts are cutaneous or mucosal growths in the genital region and around outlets such as the anus, most commonly caused by infection with the human papillomavirus (HPV). These lesions may appear as single or multiple growths, either small and cauliflower-like or flat and smooth, with considerable variation in size and shape.
The anorectal region and genital areas contain delicate skin and mucosa that are in close contact with each other; viruses transmitted through skin-to-skin or sexual contact can easily penetrate these surfaces and induce localized growths. In addition, the distinction between mucosa inside the anal canal and skin outside is important when choosing treatment and predicting discomfort.
The primary cause is human papillomavirus (HPV). Multiple HPV types exist: some are “low-risk” and mainly cause warts, while others are “high-risk” and associated with genital cancers. Most externally visible warts are produced by low-risk types and are not cancerous by themselves; however, the presence of HPV implies transmissibility, and in some cases the coexistence of high-risk types is possible—making follow-up and prevention essential.
The clinician will ask about symptoms, time of onset, sexual partners, prior history of warts, and previous treatments, followed by a careful examination of the skin and mucosa in the affected area.
The goal of treatment is typically to remove the visible lesions (warts) and reduce symptoms and viral transmission. Treatment does not necessarily eradicate the virus itself, and recurrence remains possible.
Note: All of these medications must be prescribed by a clinician. Incorrect or unsupervised use can cause significant irritation or tissue injury. Several of these agents are contraindicated during pregnancy.
Yes. Even after visible lesions are removed, the virus may persist in the skin or mucosa, allowing new lesions to appear later. Some individuals experience repeated recurrences and may require multiple treatments or long-term follow-up.
Seek medical attention immediately or as soon as possible if:
No. If the lesions are small, asymptomatic, and few in number, a watchful waiting approach is acceptable. Treatment is recommended when there is discomfort, bleeding, or patient concern.
No treatment completely eliminates the virus; however, therapy removes visible lesions and reduces symptoms. Recurrence remains possible.
In most cases, partners should be informed and advised to seek evaluation and counseling. Many national guidelines recommend that current or recent sexual partners be notified and assessed. The need for testing or treatment depends on individual circumstances and the clinician’s recommendations.
Yes. The vaccine helps prevent new HPV infections and, in many cases, reduces the risk of acquiring additional HPV types. Your clinician can provide individualized guidance based on your situation.
It is advisable to avoid sexual contact—or use condoms consistently—until visible, potentially transmissible lesions have resolved and treatment is complete, preferably with your clinician’s confirmation. Open communication with your partner is important.
Anal warts are a common condition caused by HPV and are often treatable with local, office-based procedures. The condition is both common and manageable, although the virus may persist in the body and recurrences can occur. Preventive vaccination and safer sexual practices (limiting the number of partners and proper condom use) are the most effective preventive strategies.
A range of treatment options exists—from topical medications to cryotherapy and surgical excision—selected according to the size and location of the lesions and patient preference.
In pregnancy and immunocompromised individuals, treatment choices differ, and consultation with a specialized care team is essential.