
Laser Treatment Center for Anal Conditions
Colorectal Cancer Treatment Center
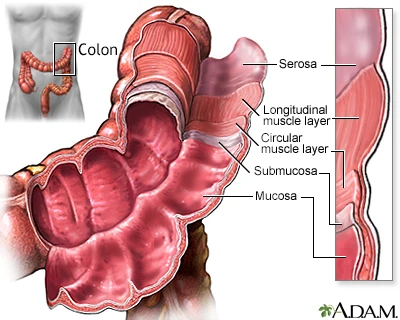
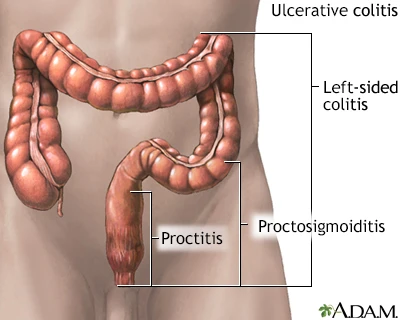
Ulcerative colitis is a chronic inflammatory disease of the large intestine where the inflammation is limited to the mucosa (superficial layer) of the colon and typically begins in the rectum, spreading continuously upwards. In simple terms: the disease location is always in the colon, and unlike Crohn’s disease, the full thickness of the intestinal wall is not involved.
The exact cause is unknown, but a combination of three main factors plays a role in the development of the disease:
Dysregulated immune response — The immune system shows an abnormal reaction against the intestinal mucosa, leading to chronic inflammation.
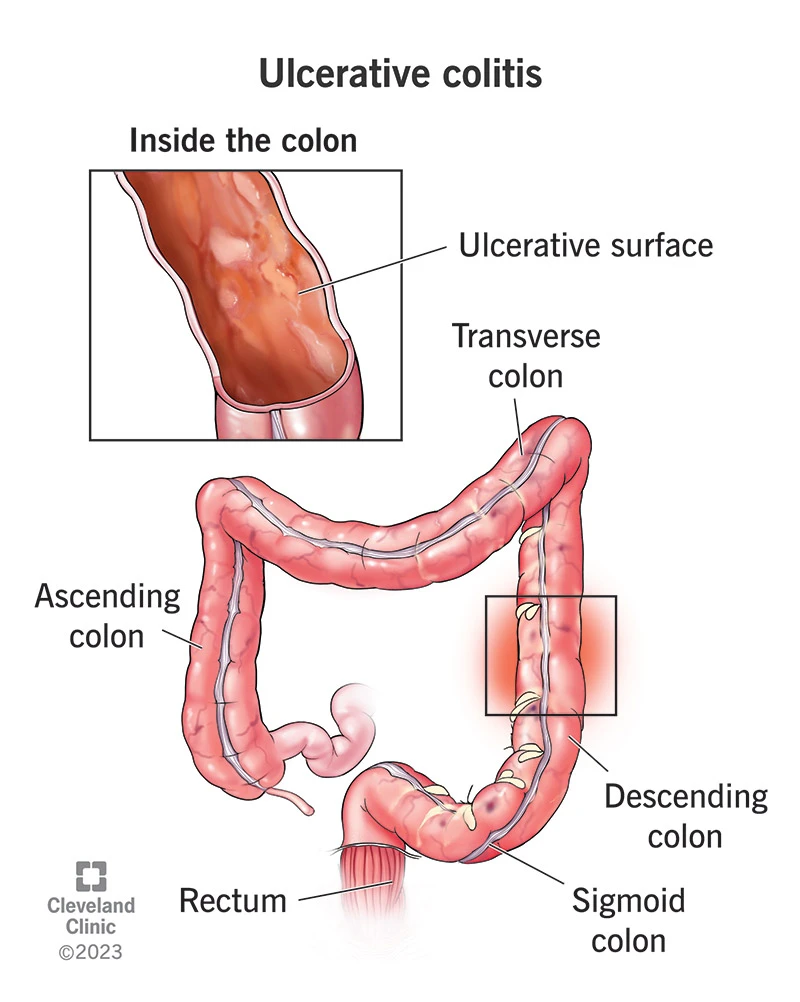
In ulcerative colitis, the immune system continuously targets the colon mucosa. This superficial inflammation causes redness, superficial ulcers, and mucosal bleeding. Over time, widespread inflammation can lead to the loss of portions of the mucosa and structural changes, which increases the risk of precancerous changes. The typical course is characterized by the continuous and extensive nature of the inflammation (from the rectum upwards).
Extraintestinal manifestations may include: joint pain or inflammation (arthritis), skin lesions, eye inflammation (redness or eye pain), and hepatobiliary problems (especially a co-existing condition called Primary sclerosing cholangitis (PSC), which is a biliary disease that occurs in some patients. PSC is inflammation and narrowing of the bile ducts inside and outside the liver and can lead to jaundice, skin itching, and liver-kidney complications. The importance of PSC is that its association with colitis increases the risk of colon cancer and requires closer monitoring (usually starting from the time of PSC diagnosis). If PSC is suspected, liver tests and imaging of the bile ducts (such as MRCP) are mandatory.
In severe attacks, life-threatening symptoms such as hypotension or obstructive symptoms may occur.
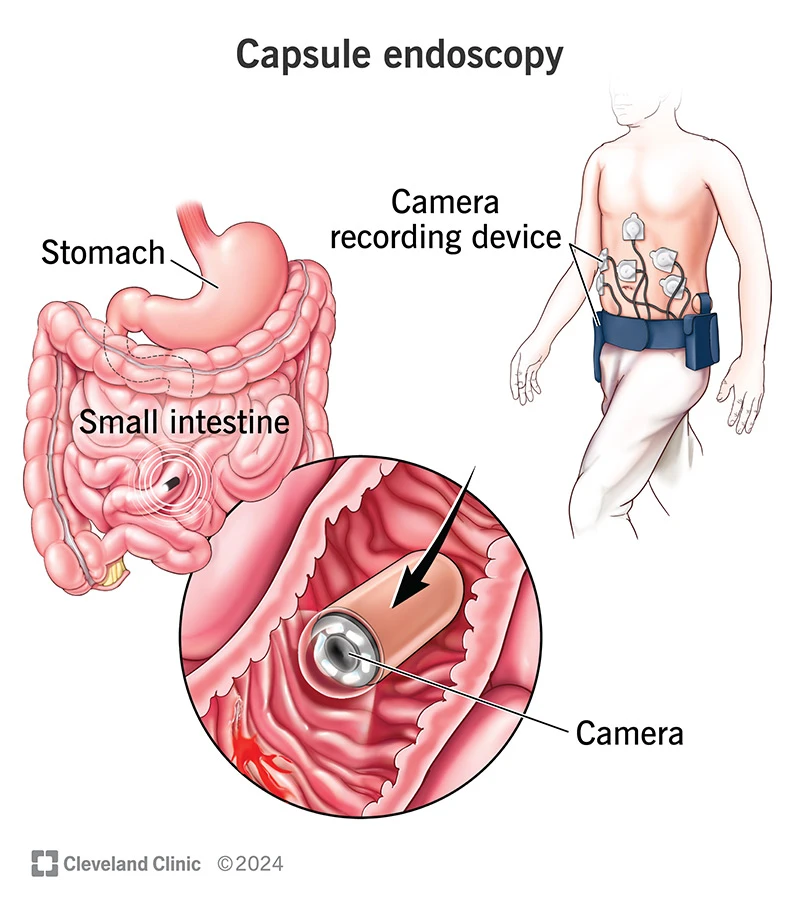
Diagnosis is based on a combination of history, physical examination, blood tests, stool tests, endoscopy, and imaging:
The main diagnostic tool. The physician closely examines the mucosa (redness, bleeding, loss of mucosal tissue) and takes tissue samples to microscopically examine inflammation and any dysplasia (precancerous changes).
CT or MRI of the abdomen/pelvis: Required in cases where evaluation of extramucosal complications (such as abscesses) is needed. These methods help to visualize the severity and extent of the involvement.
If a person has PSC, endoscopic surveillance begins at the time of PSC diagnosis and is usually more frequent (e.g., annually), as the risk of colon cancer is higher in these patients.)
Antibiotics: Generally have a limited role, except in cases of secondary infection or the presence of an abscess.
Correction of nutritional deficiencies (iron, vitamins), increasing calories in cases of weight loss, and if necessary, nutritional support (enteral or parenteral).
In life-threatening cases (toxic megacolon, bowel perforation, severe bleeding, failure to respond to intensive medical therapy), urgent or emergency surgery is required.
In refractory cases or with cancer, elective surgery is performed. The choice of surgical method is staged and based on the patient’s condition.
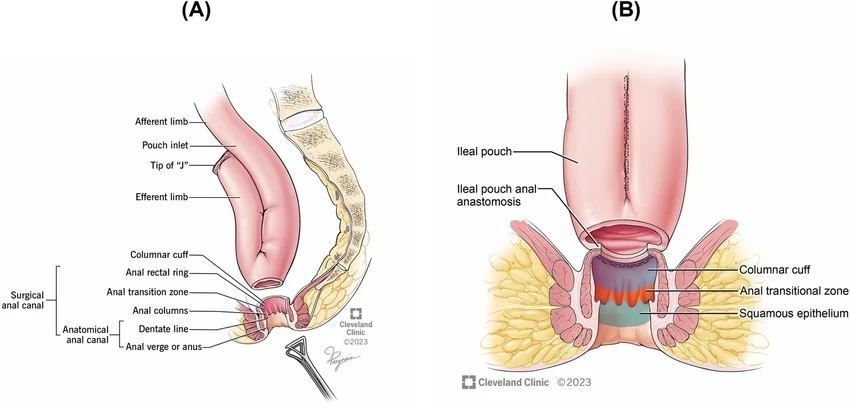
Colectomy with creation of a stoma (an external pouch) that can be temporary or permanent: In frail or emergency patients, a stoma is usually created first to stabilize the patient. In a subsequent stage, a decision can be made to construct an internal pouch or keep the stoma permanent.
Women: Colectomy and pelvic surgeries may reduce fertility by causing pelvic adhesions; if you plan to conceive, you should consult with the surgical and fertility teams before surgery. Minimally invasive techniques (laparoscopy) and protective measures may reduce this risk. In some cases, egg preservation (freezing) before surgery is recommended.
Men: The risk of nerve injury and sexual consequences is low, but if pelvic nerve tissue is damaged, sexual dysfunction may occur; nerve-sparing techniques reduce this risk.
A) Urgent indications for surgery
Toxic megacolon: When the colon becomes severely dilated; there is a risk of perforation (hole) and shock.
Perforation (bowel perforation): Requires urgent surgery for abdominal washout and infection control.
Severe bleeding that cannot be controlled with medical and endoscopic methods.
Sepsis or progressive infection resulting from bowel complications.
B) Elective indications (scheduled)
Very low quality of life: This refers to when disease symptoms—for example, more than 10 times a day, fecal incontinence, inability to work or study, depression, or social isolation due to symptoms—have been tried with all medical treatment options without sufficient results; in such cases, surgery is considered to restore function and quality of life.
“In most cases, yes; completely removing the colon usually stops colitis, but some patients still require additional treatments or follow-up care. And if a pouch is created, it may become inflamed and require treatment.
Often yes; removal of the entire colon usually stops ulcerative colitis, but some patients may need additional treatments or follow-up, and if a pouch is created, the pouch may become inflamed and require treatment.
If you have gastrointestinal symptoms (persistent diarrhea, blood in the stool, weight loss), be sure to seek medical attention; if your family has a history of early-onset cancer, request genetic counseling. Routine screening is not recommended for asymptomatic individuals without a specific family history.
In many patients with severe or recurrent symptoms, yes—surgery can resolve symptoms and improve quality of life; however, functional outcomes and potential complications must also be considered.
PSC is a biliary tract disease that can be associated with colitis; this association increases the risk of colon cancer and requires closer monitoring.
Ulcerative colitis is a chronic inflammation of the large intestine, typically associated with bloody diarrhea and urgency. Medical treatment can control the disease in many patients, but surgery is necessary in severe, refractory cases, or when precancerous changes are detected. Surgery can cure the disease (by removing the colon) or save lives in emergency situations; however, any type of surgery has its own specific consequences and complications—such as changes in bowel frequency, the risk of pouch inflammation, or effects on fertility—which will be fully discussed and planned with you before making a decision.