
Laser Treatment Center for Anal Conditions
Colorectal Cancer Treatment Center
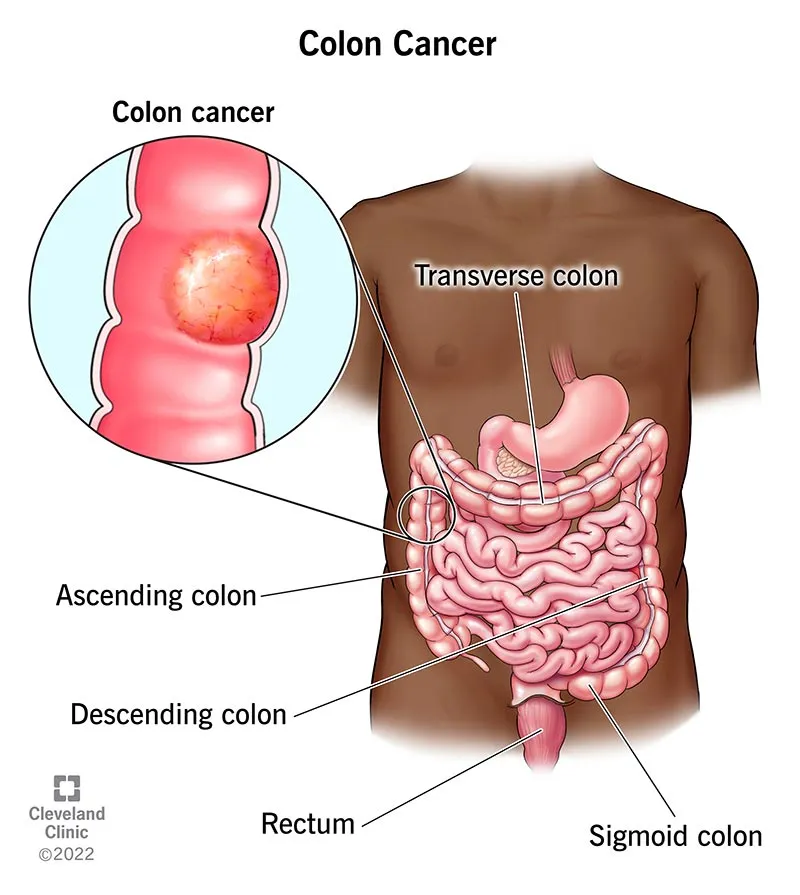
Cecal cancer refers to the development of a malignant (cancerous) tumor in the cecum, which is the first portion of the large intestine located in the lower right quadrant of the abdomen—where the small intestine (ileum) connects to the large intestine. In simple terms, it is a tumor that arises from the cells of the cecal wall and may extend into deeper layers of the bowel, spread to surrounding tissues, or disseminate to distant sites through the bloodstream or lymphatic system.
Cecal cancer, as part of right-sided colon cancers, accounts for approximately 10–15% of all colorectal malignancies. It occurs more frequently in older individuals and is often diagnosed through findings such as iron-deficiency anemia or occult gastrointestinal bleeding. According to global statistics, colorectal cancer is the second most common cancer in women and the third in men, with more than 1.9 million new cases reported annually worldwide. In Iran, colorectal cancer represents about 9–10% of all cancers and is considered one of the five most common malignancies, with an increasing trend in recent years. The exact proportion of cecal cancer within national data is not precisely defined, but most studies indicate a distribution similar to global patterns.
Cecal cancer may remain asymptomatic for a long time because the cecum has a relatively large diameter, allowing the tumor to grow without causing obstruction. This means symptoms may be mild or subtle:
In advanced cases: a palpable mass in the lower right abdomen, signs of bowel obstruction (nausea, vomiting, abdominal distension), or symptoms related to metastases—such as hepatic pain or shortness of breath if the liver or lungs are involved.
Important note: New-onset iron-deficiency anemia in an adult without an identifiable cause should prompt evaluation for a gastrointestinal source of bleeding, including colorectal cancer.
The most important and definitive diagnostic method. Using a flexible, camera-equipped scope, the physician visualizes the colon and obtains samples from any suspicious lesion. Pathology (microscopic examination) determines whether the cells are malignant.
CEA is a tumor marker that may be elevated in some patients. An increased level is not diagnostic on its own but is useful alongside other clinical information and for post-treatment monitoring.
Contrast-enhanced CT of the abdomen and pelvis is used to assess tumor extent, lymph node involvement, and possible liver metastases; chest CT is often performed to evaluate the lungs. In selected cases, MRI or PET-CT may also be used. These imaging studies determine whether the disease is localized or has spread, and are essential for treatment planning.
Assessment of the tumor’s genetic features (such as MSI status or specific gene mutations) can help guide the choice of chemotherapy, targeted therapies, or immunotherapy. In simple terms: tests that indicate which treatments are likely to be more effective.
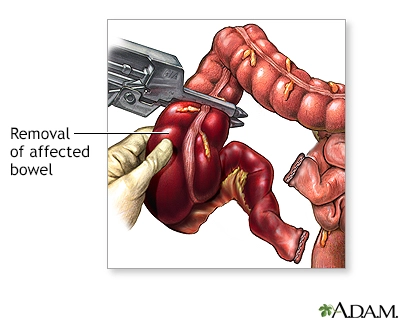
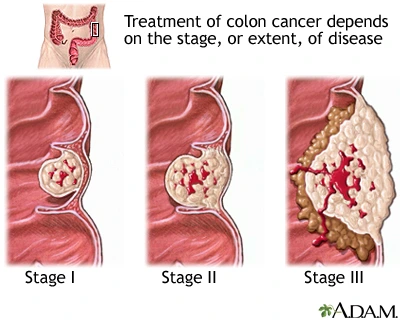
Overall goal: to remove the tumor, prevent further spread, and improve survival and quality of life.
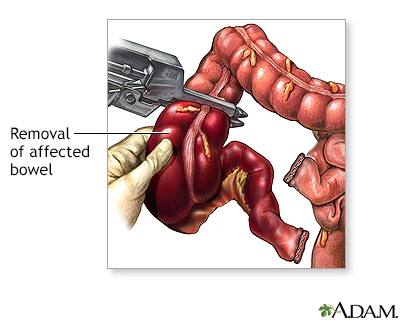
Yes — if detected early and the tumor is confined to the cecum, surgery with or without chemotherapy offers a high chance of cure. However, each case must be evaluated individually.
If a first-degree relative (parent, sibling) has been affected, or if you have a history of multiple polyps or a genetic condition, genetic counseling and a specialized screening plan are recommended. Otherwise, the general recommendation is for every adult to undergo routine colorectal screening—such as colonoscopy or other approved screening tests—according to local guidelines.
No; many gastrointestinal conditions can cause these symptoms, but any new or concerning symptom should be medically evaluated to determine the exact cause.
Right hemicolectomy generally does not have a significant impact on fertility in women (unlike surgeries performed deep within the pelvis). However, if you have concerns, you should discuss them with the surgical team before the operation so that appropriate planning can be made.
Depending on the surgical approach (laparoscopic or open), your overall condition, and the presence of any complications, recovery usually takes from several weeks to a few months. The surgical team will guide you regarding the appropriate time to return to work and resume normal daily activities.
Cecal cancer is a tumor that develops in the first part of the large intestine. It may begin with fatigue and anemia, and in more advanced stages can present with pain or changes in bowel habits. Definitive diagnosis is made through colonoscopy and biopsy; surgery is the main treatment, with chemotherapy or targeted therapies added in certain stages. The earlier the tumor is detected, the better the chance of recovery. If you experience unexplained fatigue, weight loss, or gastrointestinal bleeding, be sure to consult a physician.