
Laser Treatment Center for Anal Conditions
Colorectal Cancer Treatment Center
Functional constipation, also known as obstructed defecation syndrome (ODS), refers to a condition in which a patient is unable to effectively empty the rectum despite feeling the urge to defecate.
The hallmark symptoms include prolonged straining, a persistent sense of incomplete evacuation, the need for manual assistance (digitation) to help pass stool, and spending excessive time on the toilet.
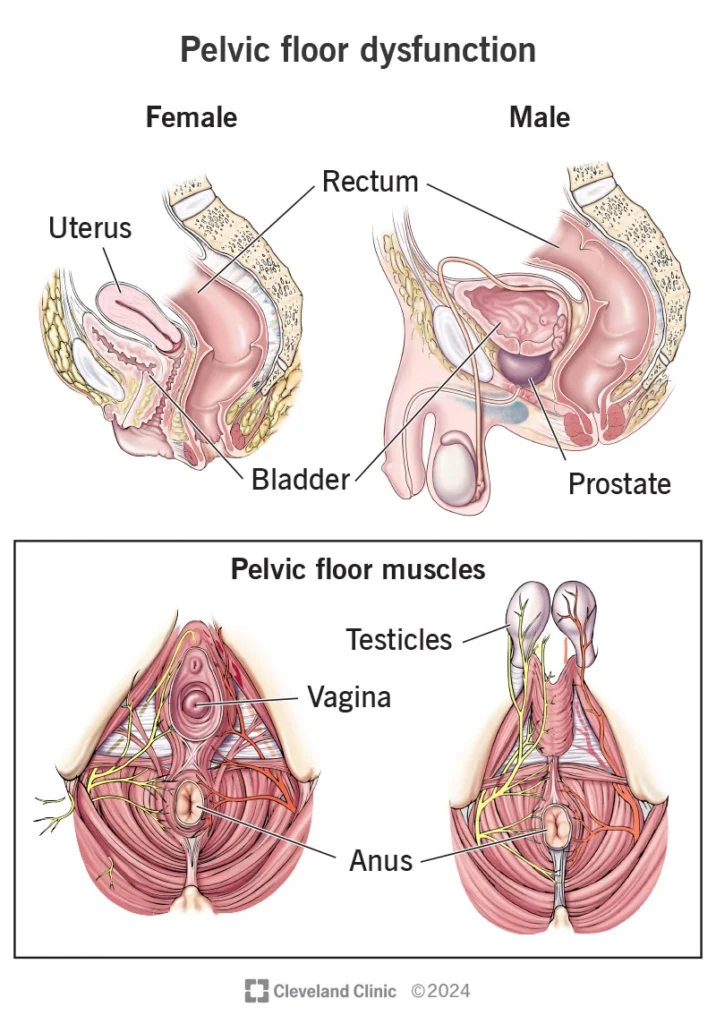
In this syndrome, both functional problems of the pelvic floor muscles (such as dyssynergia) and anatomical abnormalities—including rectocele, mucosal prolapse, or intussusception—may be present.
Therefore, diagnosis and treatment must be multidisciplinary and combined, addressing both functional and structural components.
ODS is one of the common forms of chronic constipation.
Although prevalence varies across studies in developed countries, a significant proportion of patients with chronic constipation—up to 20–30% in some populations—report symptoms of inadequate evacuation or excessive straining. The condition is more frequent in women, particularly those with a history of childbirth, and is seen more often in middle-aged and older adults.
Dyssynergia, or lack of coordinated relaxation of the pelvic floor muscles and anal sphincter during defecation (anismus)
In many patients, a combination of multiple factors occurs simultaneously, which is why a comprehensive evaluation is essential.
All of these mechanisms may cause symptoms individually or in combination, which is why a simultaneous assessment of both functional and anatomical factors is essential.
Diagnosis of ODS requires a combination of history-taking, physical examination, and functional/imaging studies.
The usual sequence and practical considerations are as follows:
(Step-by-Step Management Guide)
Before any invasive intervention—especially surgery—the patient should undergo at least three months of medical therapy and defecation retraining, including biofeedback.
Advantages / Limitations: Provides early symptom relief; short-term improvement is reported in 70–90% of patients. However, long-term outcomes show recurrence rates of 30–40%, emphasizing the need for careful patient selection. Rare but significant complications—such as major bleeding or persistent pain—have been reported.
(For patients at risk of incontinence or when LIS is not appropriate)
No. Small rectoceles without symptoms—or those causing only mild constipation—are usually managed with medical therapy and pelvic floor physiotherapy.
Surgery is considered only when the rectocele is large, clearly associated with incomplete evacuation, and unresponsive to biofeedback.
Biofeedback typically involves 6–12 sessions, held weekly or every two weeks, along with home exercises.
Many patients notice early improvement after just a few sessions, but completing the full course is important for long-term skill reinforcement.
Evidence shows that biofeedback is effective and is considered the first-line treatment for dyssynergia.
Both have advantages and limitations.
Fluoroscopic defecography is less expensive, provides real-time imaging, and is very useful for assessing evacuation mechanics.
MRI defecography avoids radiation, offers superior soft-tissue detail, and visualizes all three pelvic compartments simultaneously.
Studies show no absolute superiority of one method over the other; the choice depends on availability and the experience of the center performing the test.
The next step depends on imaging and manometry findings.
If a correctable anatomical problem is present, a targeted surgical procedure—such as LVMR or STARR in selected cases—may be considered.
These decisions are made within a multidisciplinary team to ensure the most appropriate and effective treatment plan.
The goal of surgery is to improve quality of life and make evacuation easier.
Some patients experience significant improvement, while others achieve only partial relief.
Proper patient selection and the experience of the surgeon play key roles in determining the final outcome.
Functional constipation, or ODS, refers to difficulty emptying the bowels, which may result from pelvic floor muscle dysfunction or from anatomical problems such as rectocele or prolapse.
The first and most important step in management is always non-surgical therapy and rehabilitation, particularly biofeedback.Dynamic imaging and functional tests help identify the primary cause. Surgical options are considered only when conservative treatments fail and a correctable anatomical abnormality is present. Decision-making should involve a multidisciplinary team—including an experienced colorectal surgeon, a radiologist, and a pelvic floor physiotherapist—to ensure the best possible outcome.