
Laser Treatment Center for Anal Conditions
Colorectal Cancer Treatment Center
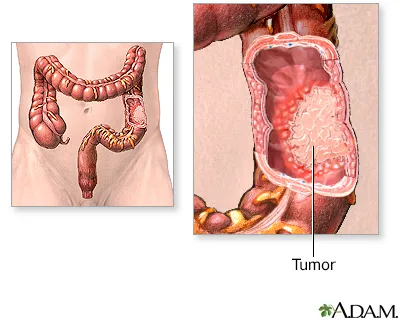
Sigmoid colon cancer is a malignant tumor that arises from the mucosal lining of the sigmoid segment of the large intestine—the S-shaped portion located near the rectum. The tumor may initially grow without noticeable symptoms, then progressively invade deeper layers of the bowel wall, involve regional lymph nodes, and metastasize through the bloodstream or lymphatic system to other organs such as the liver or lungs.
Sigmoid colon cancer is one of the most common types of colorectal cancer, accounting for approximately 25–30% of all cases. Because of its proximity to the rectum, it often presents with symptoms such as visible bleeding, changes in bowel frequency, or a sensation of incomplete evacuation, and therefore tends to be diagnosed earlier than more proximal colon cancers.
Globally, the sigmoid colon is among the most frequently affected sites, and data from Iran show a similar pattern. National statistics indicate that a substantial proportion of colorectal cancer patients in Iran have sigmoid tumors, and the average age at diagnosis is lower compared with Western countries.
A benign protrusion (polyp) may form in the colonic mucosa. Most polyps are harmless, but some—especially adenomatous polyps—have the potential to transform into cancer.
Over the course of years, mutations develop in genes that regulate cell division and DNA repair (for example, mutations in various molecular pathways). These changes lead to abnormal cellular behavior.
As mutations accumulate, the polyp can evolve into an invasive tumor that penetrates from the mucosa into the muscular and outer layers of the bowel wall.
Tumor cells may enter lymphatic or venous vessels and disseminate to lymph nodes, the liver, lungs, or other organs.
Key point: This process usually takes many years; therefore, detecting and removing polyps during colonoscopy is an effective preventive measure.
Any persistent symptom, or symptoms accompanied by weight loss or anemia, requires prompt evaluation.
1.Colonoscopy with biopsy:The gold standard for diagnosis. The lesion is directly visualized, and a biopsy is taken for pathological confirmation.
2.Blood tests: CBC to evaluate for anemia; liver function tests (to assess possible liver involvement); and CEA for post-treatment surveillance.
3.Staging imaging (contrast-enhanced CT of the chest, abdomen, and pelvis):Used to determine tumor extent, assess for suspicious lymph nodes, and detect liver or lung metastases.
The imaging report should specify whether liver lesions are single or multiple, their location within hepatic segments, and whether there is evidence of tumor invasion beyond the bowel wall.
4.Molecular pathology testing: MSI/MMR testing and mutation analysis such as KRAS/NRAS/BRAF, which influence the selection of targeted therapy or immunotherapy.
5.In selected or complex cases: MRI or PET-CT may be performed for more precise evaluation of local disease or metastatic spread.
Key criteria: Number, size, and location of liver lesions Ability to remove all lesions or combine resection with ablation Response or lack of response to systemic chemotherapy Absence of uncontrolled widespread disease elsewhere
Overall patient condition and liver function In many cases, initial chemotherapy is given to shrink the lesions (downsizing) and reassessment is performed to determine whether liver resection is feasible. The final decision is made by a multidisciplinary team.
Yes. A high-fiber diet, reducing processed meats, maintaining a healthy weight, and regular physical activity can help lower the risk and support recovery after treatment.
Not necessarily. In many patients, if the liver lesions are removable or can be controlled locally and overall health allows it, surgery or local treatments for liver metastases may still be performed with curative intent. The decision depends on detailed evaluation by a multidisciplinary team.
Usually one year after the operation; if the result is normal, the next exam is done after 3 years and then every 5 years, depending on the findings.
Many patients return to normal life after recovery, but depending on the extent of the operation, there may be changes in bowel frequency or nutritional needs. Your care team will provide detailed guidance.
High fever, sudden and severe abdominal pain, persistent or heavy bleeding, or foul-smelling discharge from the wound are warning signs and require urgent medical attention.
Sigmoid colon cancer is a condition that, in many cases, can be treated or controlled if detected early. Definitive diagnosis is made through colonoscopy and biopsy; surgical removal of the tumor is the cornerstone of treatment, and in high-risk or metastatic cases, chemotherapy, targeted therapies, or metastasectomy complement the treatment plan. Improving diet, exercising, and adhering to follow-up schedules significantly increase the chances of successful outcomes.