
Laser Treatment Center for Anal Conditions
Colorectal Cancer Treatment Center
Anal cancer is the uncontrolled growth of malignant cells in the anal canal or the surrounding perianal area. The most common type is squamous cell carcinoma, which arises from the cells lining the inner surface or skin of the anus.
This disease may present with a mass, a persistent ulcer, or bleeding in the anal region. Treatment typically involves a combination of radiation therapy, chemotherapy, and occasionally surgery.
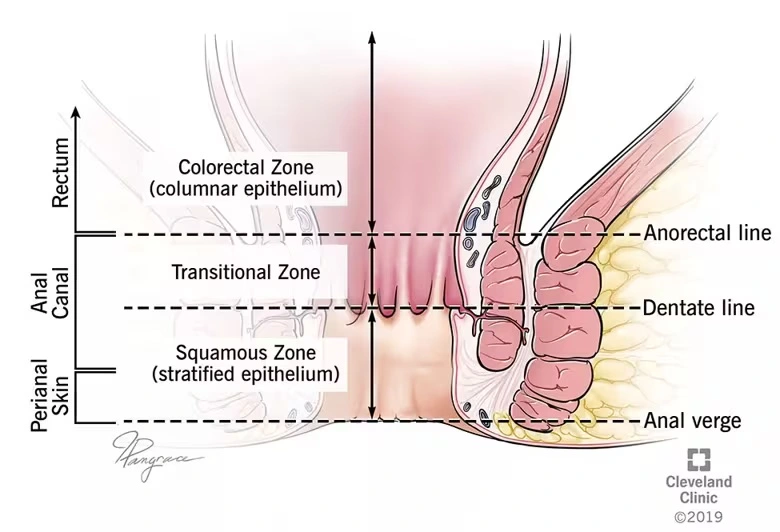
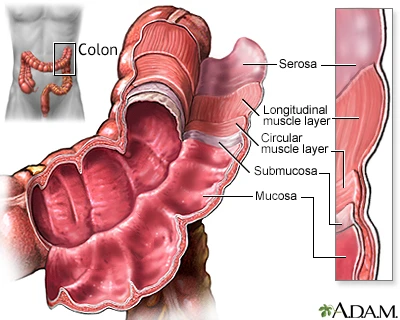
The anal canal is short and extends from the inner mucosal lining to the perianal skin. Surrounding the canal are lymphatic channels and glandular structures that may serve as pathways for tumor spread. Additionally, important lymph nodes are located on both sides in the inguinal region (groin), which may become involved.
Understanding whether the tumor originates within the anal canal or on the perianal skin, as well as the status of regional lymph nodes, is essential for selecting the appropriate treatment.
Unlike colon and rectal cancers, anal cancer is far less common and accounts for less than 2% of all lower gastrointestinal malignancies. Globally, its incidence is rising and is strongly associated with HPV infection and high-risk sexual behaviors.In Iran, precise national statistics are limited, but available reports suggest that the incidence is lower than in Western countries. Nevertheless, the increasing prevalence of HPV-related cases indicates that its numbers may rise in the coming years.
Key point: HPV infection alone does not necessarily cause cancer, but it significantly increases the risk; therefore, surveillance in high-risk groups is important.
The process typically follows this pattern:
Chronic infection with high-risk HPV types leads to cellular changes in the superficial lining of the anal canal (disruption of pathways that regulate cell division and DNA repair). Over time, some of these changes progress to cellular abnormalities and eventually malignancy.
This progression may take years, which is why prevention and surveillance in high-risk groups are essential.
Treatment decisions are made within a multidisciplinary team, including a colorectal surgeon, radiation oncologist, medical oncologist, radiologist, and pathologist.
The cancer itself is not “contagious.”
However, its main risk factor—HPV—is a sexually transmissible virus.
HPV infection in a person means the virus can be transmitted, but cancer develops only after a long, multi-step process, and HPV infection alone does not mean cancer will occur.
No. Most HPV infections clear on their own or cause only benign conditions such as warts.
Only a subset of infections—especially those involving high-risk HPV types and persisting over time—can lead to precancerous changes and eventually cancer.
No. In many cases, the initial combination of radiation therapy and chemotherapy can eradicate the tumor while preserving the anus and sphincter.
Removal of the anus (APR) is usually necessary only when the tumor does not respond adequately to initial treatment or when a local recurrence occurs.
The HPV vaccine is preventive. It has been proven to prevent initial infection with the HPV types included in the vaccine.
In some individuals, it may reduce the risk of new HPV infections, but its most clearly established benefit is in people who have not yet been exposed to those HPV types.
Consulting a physician can help determine what is appropriate in your specific situation.
People living with HIV may present with more advanced tumors or may respond differently to treatment.
Optimal control of HIV and close coordination among specialists are essential.
More frequent and careful follow-up is recommended in many centers to ensure the best outcomes.
Yes. Pelvic radiotherapy can affect fertility, for example by reducing ovarian reserve or damaging sperm production.
If future fertility is important to you, discuss fertility preservation options—such as sperm freezing or egg/embryo freezing—before starting treatment with your care team and a fertility specialist.
If you notice a new lump or persistent ulcer in the anal area that does not heal within a few weeks, unusual bleeding, severe pain, swelling in the groin, or general symptoms such as fever or rapid unexplained weight loss, you should seek medical attention promptly.
Anal cancer is a condition that, in many cases, can be controlled—or even cured—when detected early and treated appropriately.
HPV infection is a major contributing factor and can often be prevented through vaccination and safe sexual practices.
Treatment decisions are usually multidisciplinary and aim to achieve the best chance of cure while preserving anal function whenever possible.
If you notice a new lump or ulcer, or experience changes in bowel habits or bleeding, seek medical attention as early as possible.